

Study by Tufts CSDD uncovers potential reasons behind CRA shortages, turnover, experience requirements, and more.
The COVD-19 pandemic and changing global economies have impacted the clinical research workforce resulting in attrition, shortages, and staffing challenges. Current workforce shortages have posed numerous hurdles for clinical research stakeholders, including sponsors, investigative sites, contract research organizations (CROs), and industry associations.1 The role of the clinical research associate (CRA) has been especially affected as high rates of turnover and vacancies proliferate. CRA turnover rates have been reported as high as 30% in the US with similar rates noted globally.2
Recent research has examined current approaches to CRA training, performance assessment, and experience. The results of a global survey of 661 clinical research professionals, including 52 CRAs, assessing their own competencies indicated that respondents with more post-secondary education reported higher levels of self-confidence in their research skills and those professionally certified by the Association of Clinical Research Professionals (ACRP) and/or Society of Clinical Research Associates (SOCRA) compared to those who were not. Self-confidence also increased with the level of academic degree.3 Researchers used a Joint Task Force (JTF) for Clinical Trial Competency Framework to assess respondents on eight competency domains. The results are consistent with prior research conducted in 2016.4
The JTF for Clinical Trial Competency framework as discussed by ACRP “objectively defines the knowledge, skills, and attitudes necessary for conducting safe, ethical and high-quality research.”5 Although common practice is currently to hire CRAs with two years of experience, high demands, vacancies, and attrition in the industry have led researchers to recognize a need to address the two years of required experience for those entering the clinical research workforce. Proposed solutions include conducting outreach to raise awareness of the profession, capturing measures of experience and transferable skills as well as add to competency-based training and innovative recruitment and retention approaches to attract candidates to the field.5
An examination of the entry-level shortage of CRAs cites several factors including the requirement of a minimum of two years of work experience, high CRA turnover, increasing numbers of open CRA positions, and clinical trial growth and complexity. An assessment of a monitoring simulation of 579 CRAs from a global CRO indicates no difference in performance regardless of CRA seniority and years of experience.6,7 The research also discusses that addressing the requirement of two years of experience for CRA roles would alleviate the current shortages in the workforce.
Given the impact of the changing clinical research industry on CRAs, Tufts CSDD investigated the current role of the CRA and critical issues including shortages and turnover, and approaches to CRA training and required experience. Also, the study examined the industry practice of two years’ experience as a hiring requirement and its relationship to CRA performance and recruitment and retention practices.*
*This research study was funded by Virb, Inc.
Methodology
The research used a dual methodology comprised of a web survey of pharmaceutical, biotechnology and CRO executives and an executive roundtable with industry experts. Tufts CSDD conducted an online survey prior to the meeting to gauge perceptions and insights about the role of the CRA based on a small group of clinical research professionals from the US Areas examined included years of experience required to become a CRA and type and effectiveness of training provided. In addition, the survey gathered perceptions about CRA shortages and attrition, most successful recruitment approaches and frequently used retention strategies. CRA assessment and performance were also investigated.
A roundtable meeting was held in October 2022 with 33 participants from biotechnology and pharmaceutical companies, CROs, academia, consulting, and technology. Participants provided their insights and perceptions across a broad range of topics including CRA assessment and training and the industry standard of requiring two years of work experience as a prerequisite to hiring. Other areas explored included recruitment and retention practices; the investigative site perspective; and the impact of outsourcing models, technology, and economic factors on the CRA role.
CRA survey demographics
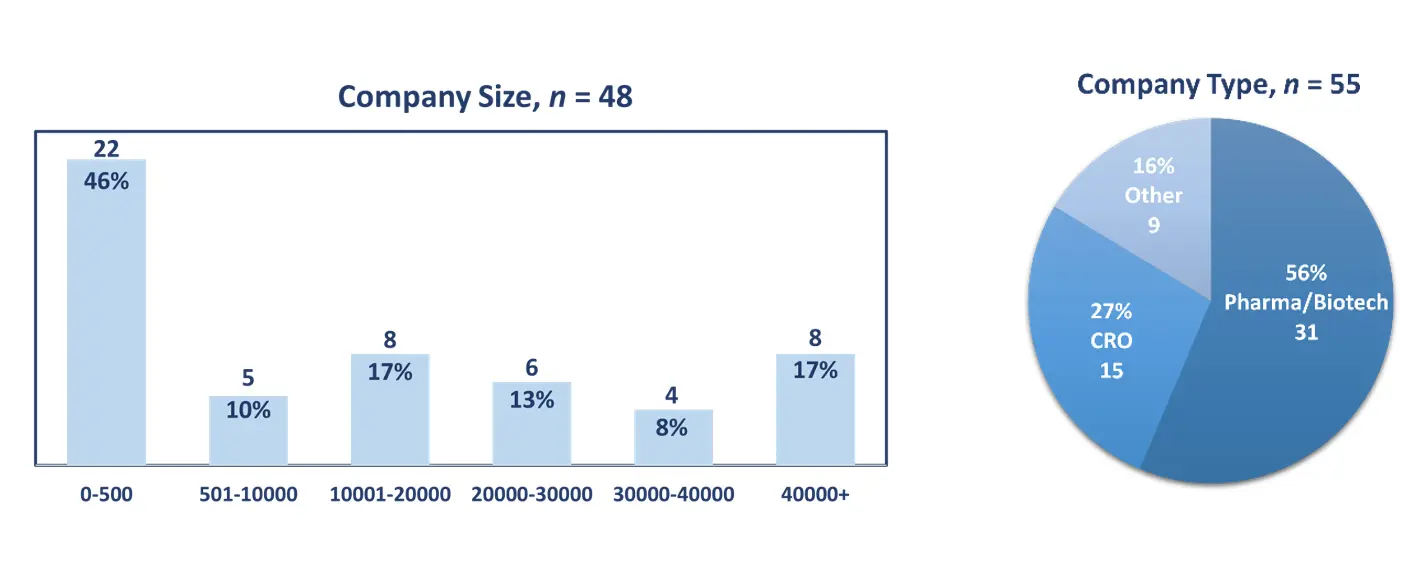
The survey was distributed via a link to an e-mail invitation using Qualtrics software to industry executives in the US primarily working in clinical operations or clinical development. A total of 55 responses were collected between August and September 2022. Respondents represented a mix of company types with over half (56%, n=31) representing pharmaceutical or biotechnology companies; more than one-fourth (27%, n=15) from CROs and 16% (n=9) from other company types. The mean number of company employees was 17,581 with companies ranging in size from 4 to 95,000 employees. Respondents had 21 years of experience on average and an overwhelming majority (91%, n=50) identified their functional area as clinical operations or clinical development.
CRA assessment
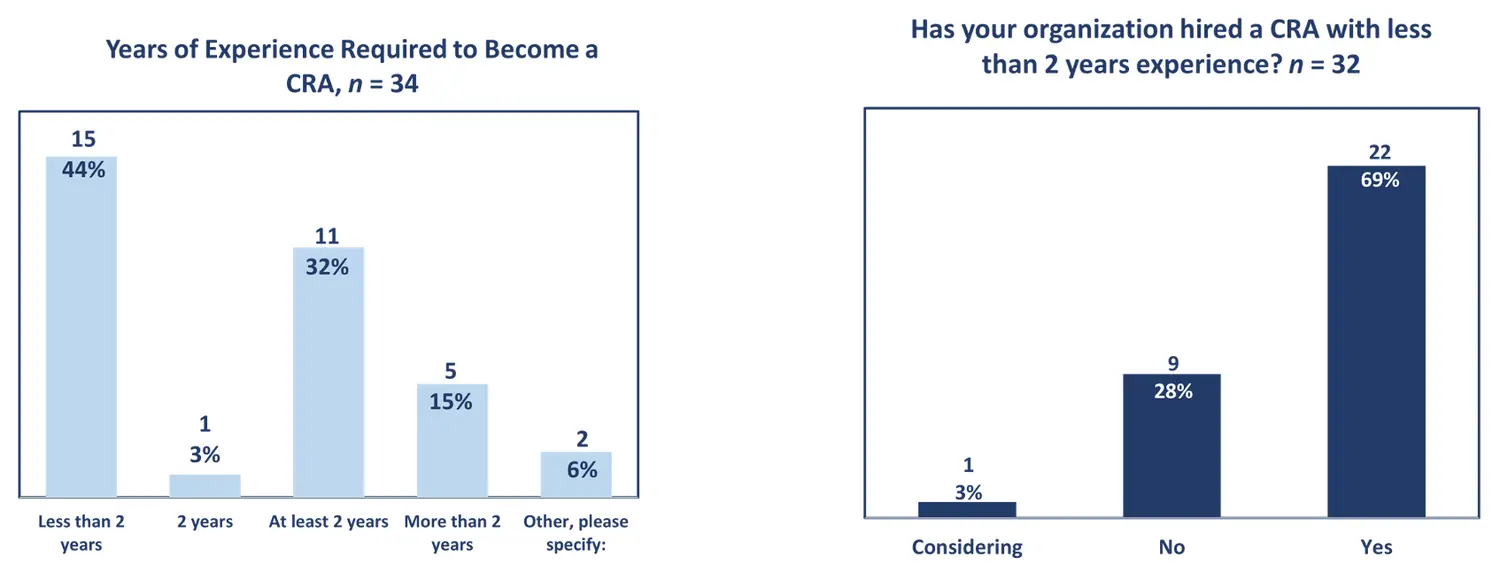
Survey responses varied regarding the number of years of experience required to become a CRA at respondent organizations with less than half (44%, n=15) indicating less than two years of experience, while more than one-third (35%, n=12) reporting two years of experience. A smaller percentage (15%, n=5) noted more than two years were needed, and a few respondents (6%, n=2) provided other responses. A majority (69%, n=22) reported that their organization has hired a CRA with less than two years of experience, while fewer (28%, n=9) did not or were considering this option (3%, n=1).
One area that emerged from the discussion was whether the current metrics used by organizations are useful and how to accurately measure CRA competency. The group discussed the implications of published data revealing that newer CRAs performed better on a simulation than experienced CRAs.6,7 The results also indicated that when comparing more experienced CRAs to newer CRAs, experienced CRAs may demonstrate complacency in their roles. A meeting participant discussed the need for CRA performance metrics:
“We don’t measure much coming from CRAs. The simulation is an exciting tool. It may not be perfect, but we need something like that to give a Pass/Fail, or at least a target. Those results are miserably low. You want to see over a two-to-three-year period that your CRAs moved up in performance and then you’re looking at performance in terms of FDA audits and CRA breaches. If we don’t start, we’ll never get to that point. We’ve been looking at this for years and years.”
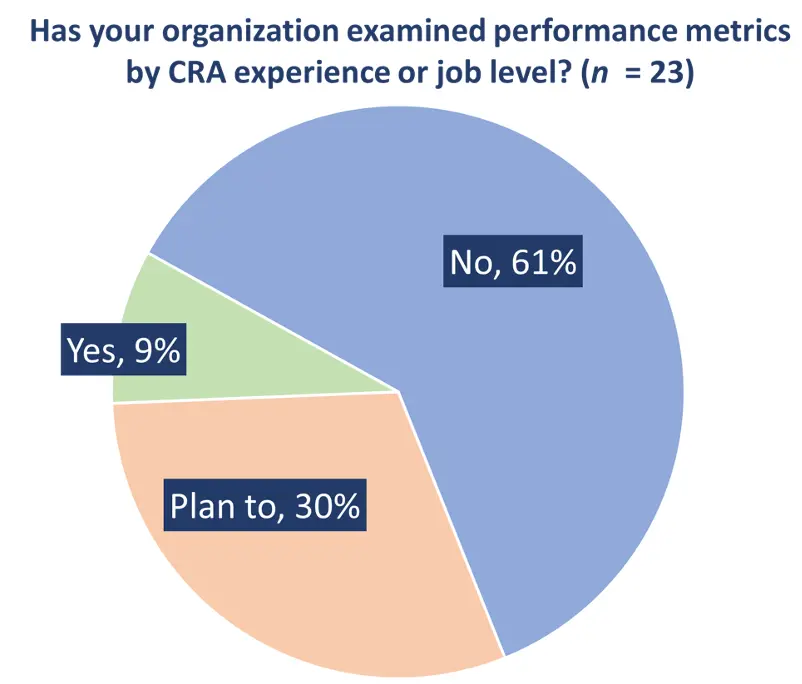
Using years of experience as the primary criteria for promotions and not performance was brought into question and participants discussed replacing years of experience as an overall performance metric. Although years of experience is currently the primary determinant of promotions, 61% (n=14) of respondent organizations have not examined CRA performance by CRA experience or job level, while fewer (9%, n = 2) have, with 30% (n = 7) planning to in the future. Enhanced pressure by organizations to promote top performing CRAs is common to prevent attrition. Focusing on other key performance indicators (KPIs), such as site satisfaction or evaluating soft skills acquired through maturity and experience were also proposed.
The group acknowledged that various therapeutic areas and phases of studies may pose different challenges for entry-level CRAs. For less experienced CRAs, trials in oncology, rare disease and gene therapy as well as larger phase III trials could potentially be difficult. Therefore, evaluating CRAs within the same therapeutic areas or phases or within one protocol might be more effective. Attendees also discussed giving CRAs access to their assessments, and building them into the CTMS system, so they can use them as a guide for improving their performance.
The investigative site perspective on the role of the CRA
Sites face multiple hurdles in evaluating CRA performance, one of which is achieving consistent performance given the difficulty with gathering metrics from newer CRAs. An added burden is that CRAs and site staff may lack training or specific skill sets required for their roles. Sites expect a CRA to provide a single point of contact to ensure responsiveness to inquiries despite CRAs often being overburdened with work.
One participant discussed the challenges to the CRA role on-site and the impact on studies:
“Study de-prioritization is a real thing that happens at sites. I can tell you this by experience. Calling CRAs and they never pick up the phone, it always must escalate to a director or manager and even then, they’re overwhelmed. Talking about site relationship managers, I have not seen one on any of our studies and the reason why sites de-prioritize a study is the sponsor or the CRO are absent. There are other sponsors who are more connected to the sites than other sponsors. If they aren’t responding or it’s taking too much effort, just put it in the back burner and let it sit.”
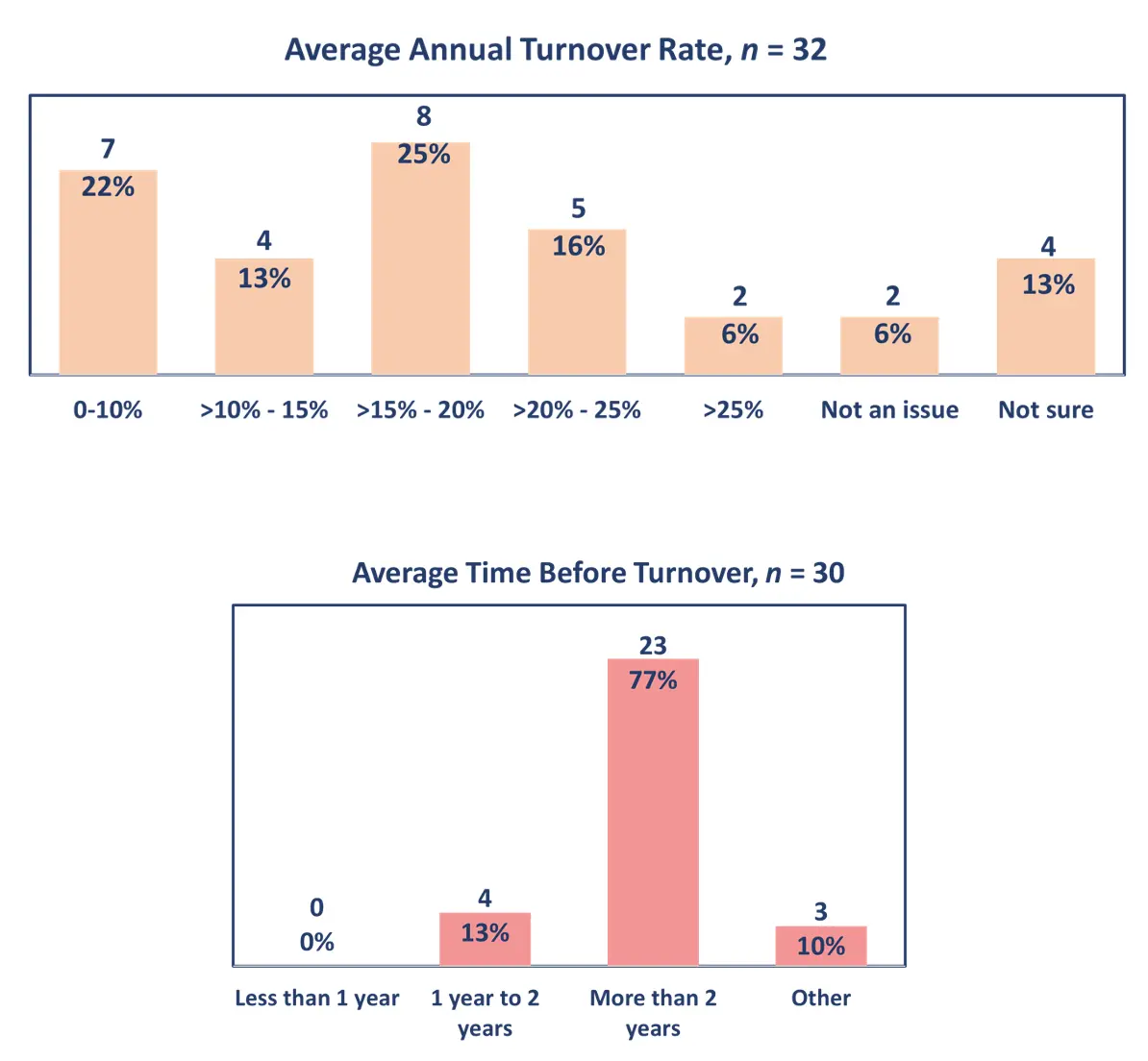
CRA turnover also impacts sites and may slow recruitment or cause study delays or terminations. Estimates of the average annual turnover rate of CRAs at organizations varied according to survey respondents. One-quarter (n=8) projected turnover between 15-20%; 22% (n=7) between 0-10%; and 16% (n=5) indicated 20-25% turnover. More than three-quarters (77%, n=23) reported that average time before turnover was more than two years.
A participant discussed “the challenge with sites is that the CRA must be the expert at all things, that resource, and it takes a CRA nine months to be proficient but they’re at a two-year cycle then that turnover is disruptive.” Senior coordinators support new CRAs and are influenced by turnover placing an even greater burden on the investigative site. A proposed solution is to have line managers work with CRAs on-site to improve rapport and teamwork.
CRA training
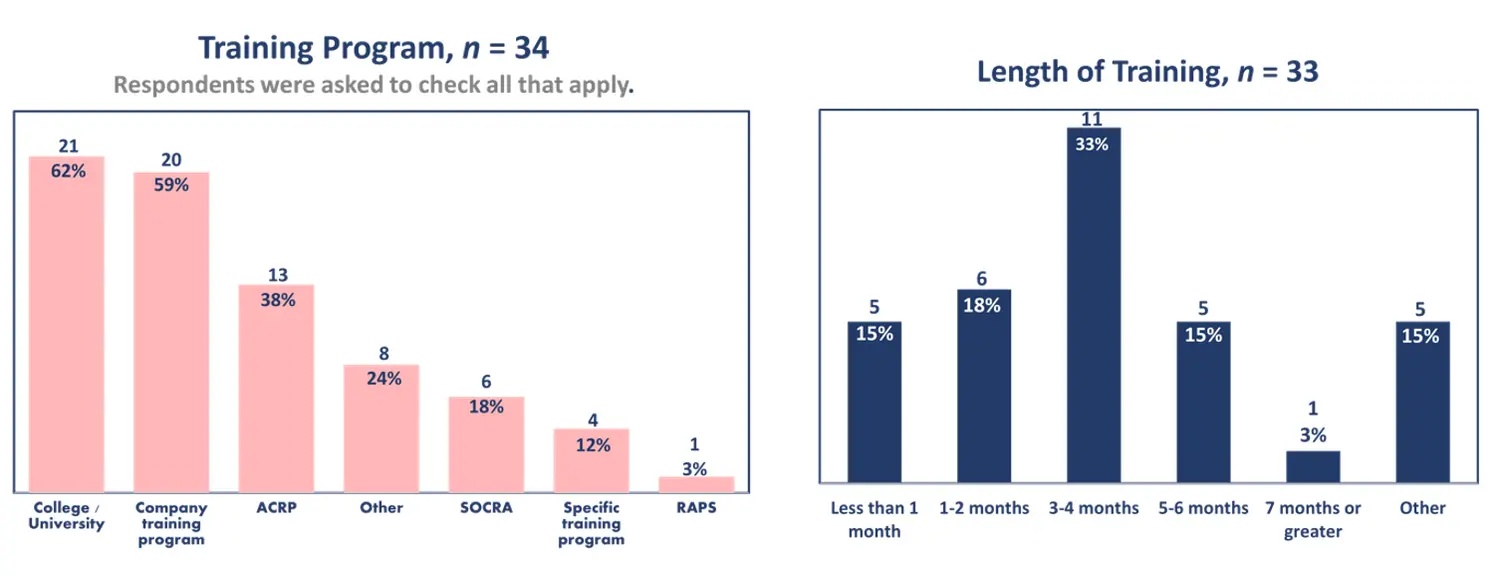
In examining where CRAs typically receive training, a greater percentage of survey respondents indicated CRAs were trained by academia (62%, n=21) or company training programs (59%, n=20). Nearly 40% (38%, n=13) reported that ACRP provided training, while fewer (36%, n=12) noted specific programs or other types. The remainder (21%, n=7) mentioned SOCRA or Regulatory Affairs Professionals Society (RAPS). More than one-third of respondents (33%, n=11) reported that new CRAs receive three to four months of training at their organization.
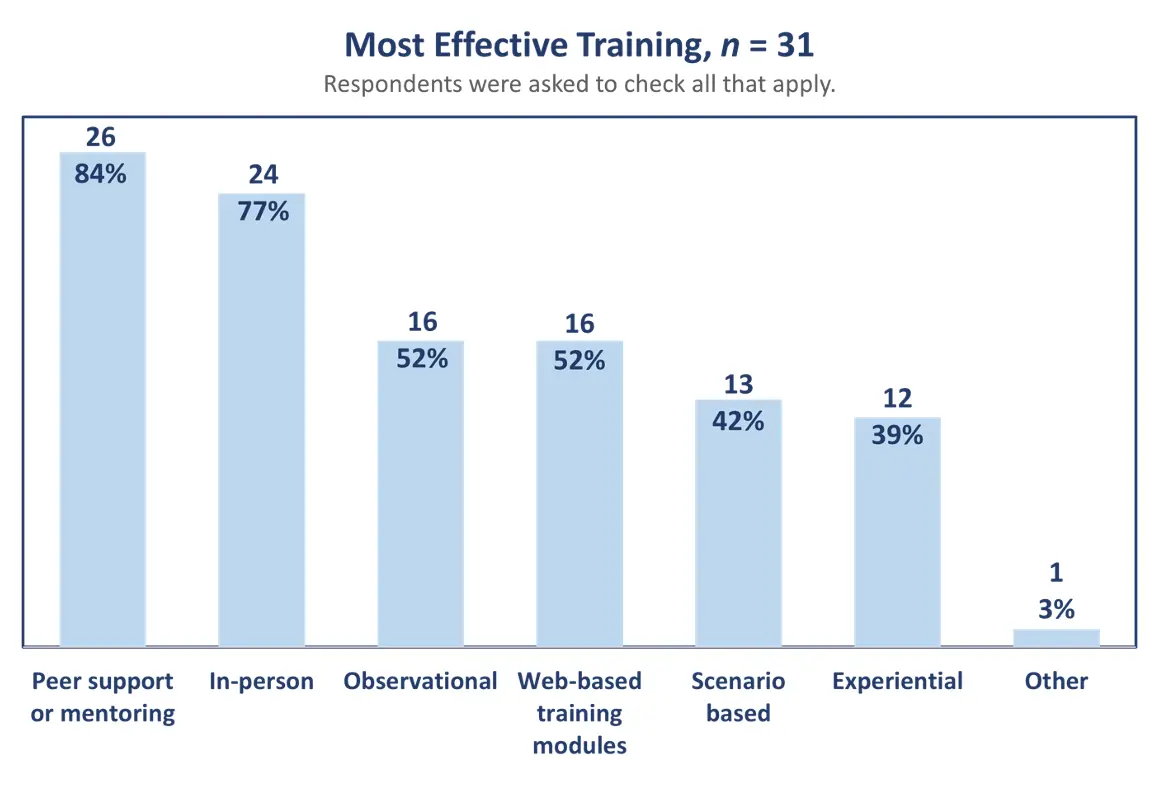
The survey also asked respondents to evaluate the most effective forms of training. An overwhelming majority of respondents (84%, n=26) reported that peer support or mentoring was the most effective training while more than three-quarters (77%, n=24) indicated in-person training was most valuable.Over half noted (52%, n=16) either observational or web-based training models were most beneficial, with 42% (n=13) reporting scenario based and 39% (n=12) experiential training. Three percent felt other trainng types were effective.
Entry-level CRA training varied at participant organizations. Some comprised large in-house training programs, while others included transitioning new college graduates from clinical study administrators to CRAs or shifting clinical research coordinators into CRA roles. Programs ranged from 12 weeks to 9 months and emphasized co-monitoring, mentoring, and training with both senior CRAs and line managers. The training also included quality assessments and use of ACRP assessments.
One participant related the details of their in-house training program:
“The demand for CRAs is growing. There’s definitely an appetite for creative ways to bring people in, we are doing that through partnership programs where you’re turning global study administrators into CRAs through a training program, including a classroom portion that is taking about three months and then actually turning into their day jobs and in another three months they’re doing on-site visits and getting that on-scene perspective.”
Companies have also established global recruitment programs for US based CRA jobs through partnerships with Mexico and Japan. A newer focus of company training emphasizes trust in partnerships. Softer skills such as communication or collaboration also comprise training and may be transferable from other roles if a candidate is new to the field.
A few alternative training approaches were proposed. One strategy included the use of chatbots for CRA questions to clarify issues and conduct training through use of behavioral data. Other methods discussed were utilizing the protocol and training documents as resources or experiential support and training.
Some general training techniques can be specifically applied to train CRAs including critical mistakes analysis of performance. This approach involves training learners on real world challenges with high stakes. Another was the use of spiral design, a training strategy intended to begin with the least complex version of a task and continue to challenge the learning with similar tasks that increase in complexity.One participant noted that “the CRA role isn’t one where individuals improve over time, but rather through training.” Attendees considered that quality of monitoring could potentially be improved through spiral learning.
Industry guidance (ICH E6R2) does not specify number of years of work experience for a CRA but stresses clinical trial specific training and experience. Nevertheless, a two-year requirement has been the industry standard and often incorporated into sponsor-CRO contractual agreements. One participant discussed that the “threshold of two years is a barrier if sponsors are not willing to take the time to train so they can provide their own help with the deficit today.” Many CROs do not have the resources to fill positions and training requires a large investment. Participants unanimously agreed that a commitment to industry training was critical.
CRA recruitment
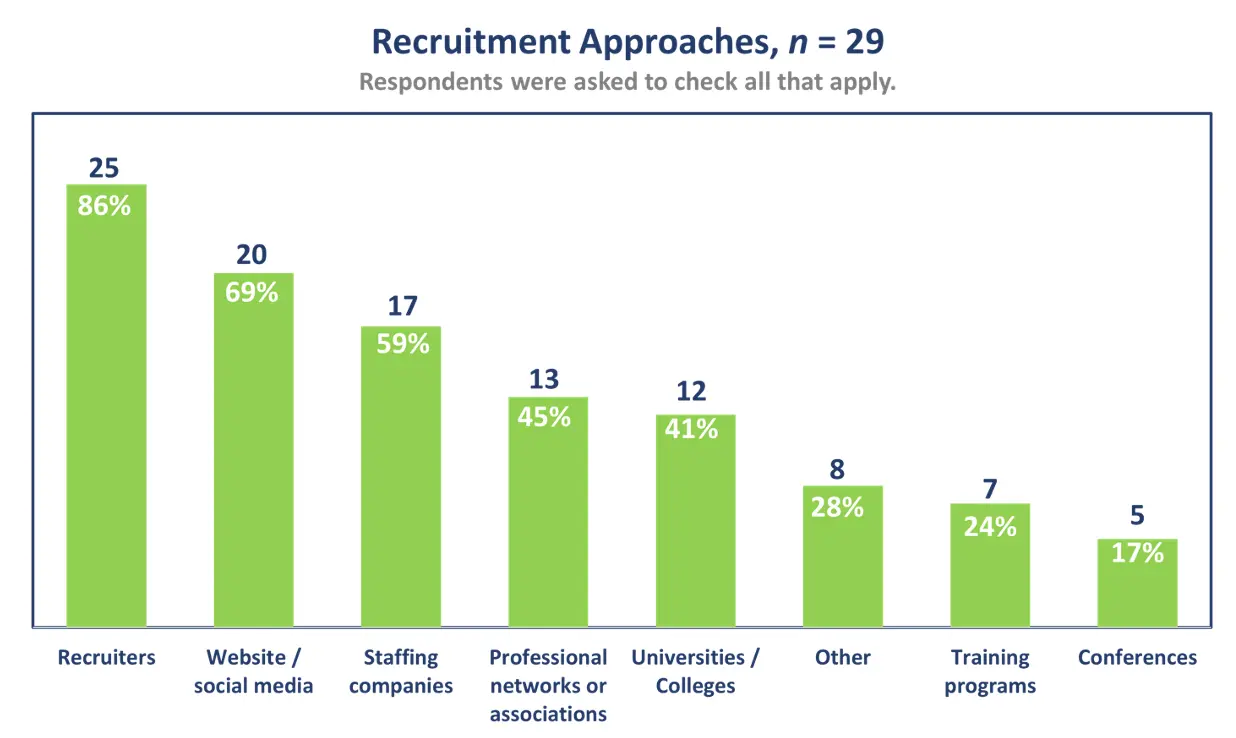
In evaluating primary CRA recruitment approaches, larger numbers of survey respondents reported using recruiters (86%, n=25), websites or social media (69%, n=20) and staffing companies (59%, n=17). Additional approaches included professional networks or associations (45%, n=13); universities or colleges (41%, n=12); and other methods (28%, n=8). Lesser numbers recruited CRAs through training programs (24%, n=7) or conferences (17%, n=5).
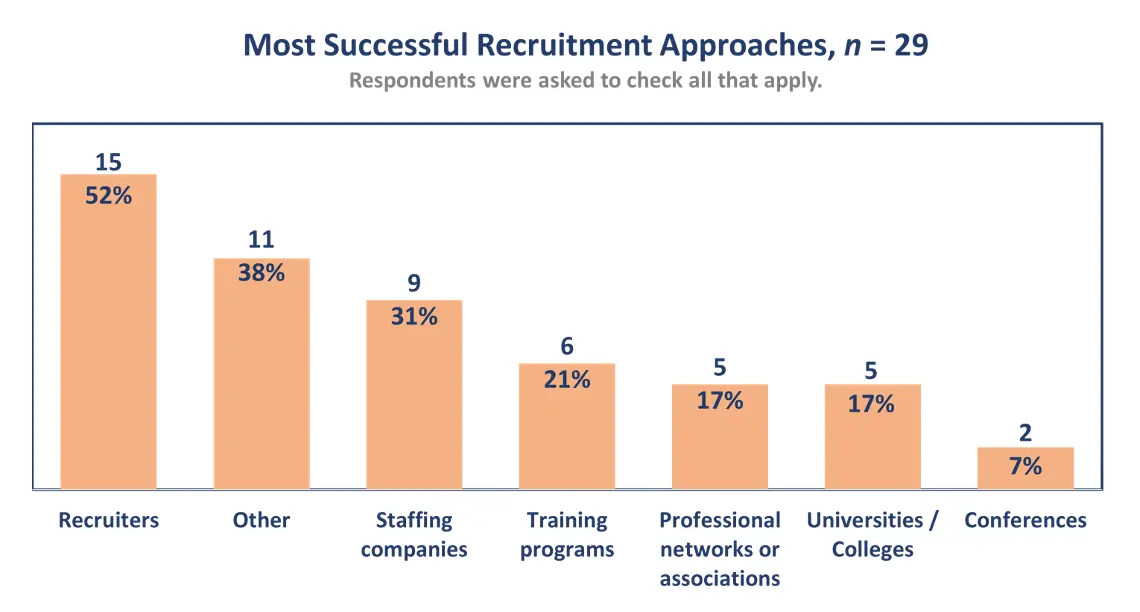
The greatest number of respondents indicated recruiters (52%, n=15) were the most successful methods of recruiting CRAs while 38% (n=11) used referrals from internal staff, recommendations or appplications. Fewer(31%, n=9) reported that staffing companies, training programs (21%, n=6), professional networks or associations (17%, n=5), universities or colleges (17%, n=5) and conferences (7%, n=2) were successful.
Academic-Industry partnerships are significant to CRA recruitment and provide extensive training through internships and fellowships. Several universities have also established clinical research programs and with demonstrated success in placing students in permanent positions. A participant from a university noted:
“We focus on getting organizations to offer cooperative education opportunities which are paid internships for preparing students not just for the working environment, but also for acquiring soft skills such as preparing their resume, write their cover letters, getting in front of companies, and engaging in the dialogues of what their experiences were.”
There is, however, a pervasive lack of awareness among undergraduate students about clinical research as a profession and of the role of a CRA. In a survey of more than 200 university students in both the US and UK, not a single one had heard of clinical research as a career.8 Recruitment by companies on college campuses over the past five years has led to some increased awareness. A meeting participant in support of recruiting new graduates explained that “the next generation wants to work for a higher purpose and what greater higher purpose than helping humanity and saving lives?” Mentoring students is also critical however, and some universities are unable to fill faculty positions due to the massive pay disparity between industry and academia.
CRA retention and perceptions about industry shortages
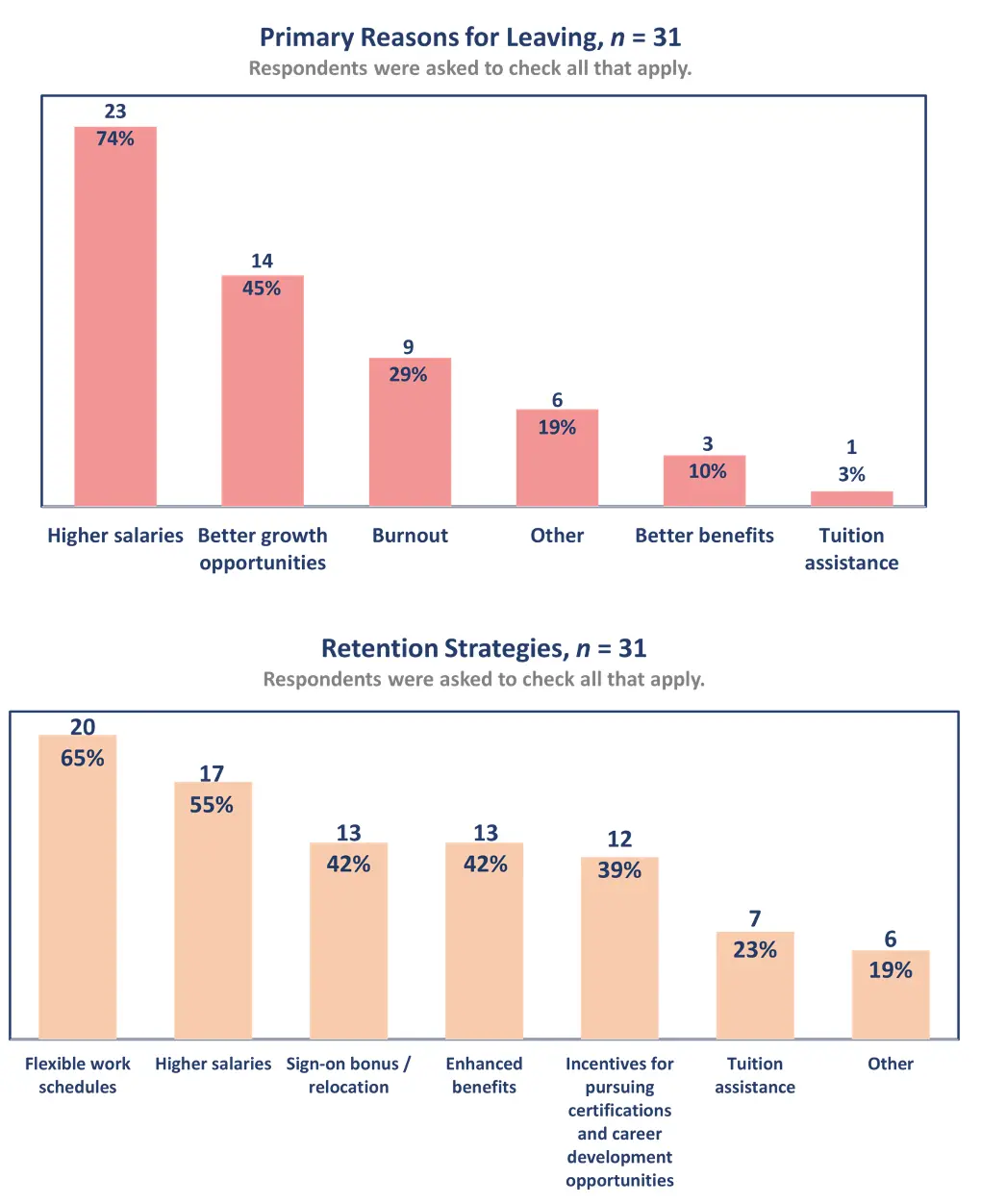
The primary reasons for CRAs leaving their positions were for higher salaries (74%, n=23); followed by better growth opportunities (45%, n=14) and burnout (29%, n=9).The top two strategies implemented by organizations were flexible work schedules (65%, n=20) or higher salaries (55%, n=17).
The growth opportunities that CRAs seek are in part impacted by the rapidly changing clinical research industry and by economic factors. Both factors influence retention of CRAs and may inhibit growth opportunities. Yearly salary increases are not sustainable, and they typically leave these roles for higher paying positions. An attendee suggested that other career paths allow a CRA to stay in the industry yet be able to advance:
“We should think about as an industry, career opportunities. What else is next? Central monitoring, data monitoring, regulatory. All require quality whether or not the role is a CRA. We want to keep CRAs while promoting, because that skill set is very valuable as a monitor.”
A CRA may experience disconnectedness from staff on-site for a number of reasons: burnout from having a large work burden; working on complex studies too soon; and managing multiple technologies and systems. One participant described the gap in the support that may contribute to a CRA feeling disconnected: “there is more separation between MDs and clinical teams, and they are not connected with the CRAs on the ground.” In addition, a CRA may currently spend less time on site and more on remote monitoring.
Company outsourced models can also influence retention of CRAs. While CROs are the primary organization that staff CRAs, pharmaceutical organizations are increasingly using internal or headcount CRAs. Participants offered mixed opinions on full service, functional service provider and freelance models. One attendee with headcount CRAs reported that turnover was less than 5%, and another indicated that functional service providers (FSP) resulted in high turnover. A third participant found no differences in performance between headcount and FSP CRAs.
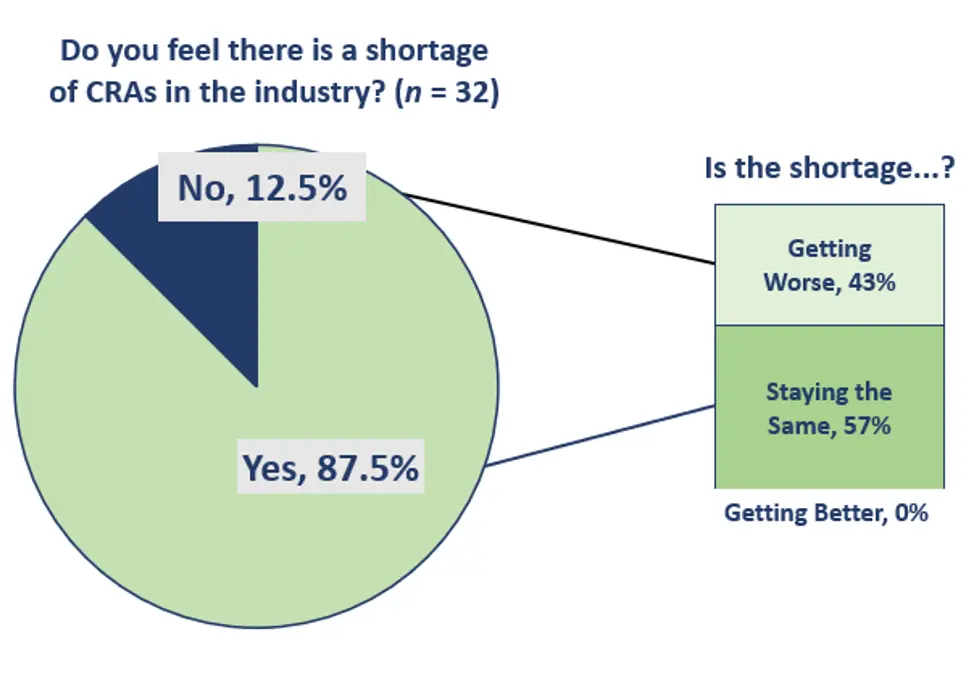
An overwhelming majority of survey respondents (88%, n=28) reported a shortage of CRAs in the industry while 13% (n=4) did not. Opinions were mixed about whether the shortage was getting worse (43%, n=14) or staying the same (57%, n=18), however no respondent felt the situation was improving.
Key findings and implications
The results of the survey and executive roundtable confirm that organizations are currently accommodating CRAs with less than two years of experience and establishing novel approaches to training. In addition, solutions are currently being implemented or planned to alleviate the impact of CRA shortages and turnover, and these include the following:
- Re-examining experience in relationship to performance through using innovative strategies to gather alternative metrics on CRA performance, such as evaluating site satisfaction or assessing soft skills.
- Organizations are also planning to link specific metrics such as FDA audits to experience or job level. In addition, evaluating CRAs with similar workloads and providing access to their assessments for self-improvement are strategies being considered. Novel approaches to gathering metrics are still in the early stages of implementation, however, and follow up studies will be critical.
- Addressing the shortage of CRAs through raising awareness of clinical research as a profession at the university level.
- Recruitment by companies on college campuses and offering university internships have led to permanent placements for students after graduation. Academic-industry partnerships also provide new graduates with valuable real-world experience before entering the workforce.
- Mentoring and working collaboratively on-site with managers can address CRA disconnectedness and facilitate teamwork as well as build trust.
- Mentoring programs provide an increased level of support for CRAs beyond training programs. In addition, dedicated line managers working on-site offer critical training. These approaches can alleviate burnout and provide the critical groundwork for encountering challenging studies.
- Providing growth opportunities to increase retention and address issues of complacency among senior CRAs as well as offering varied incentives to remain within the industry.
- A competent CRA can easily transition into other positions where comparable skills are valued and would be able to fill roles in regulatory, trial management, and central or data monitoring. Many organizations support career development of CRAs to increase staff retention.
- Given increasing use of technology and growth of decentralized trials, proposing sustainable solutions that tackle industry and global change is critical.
- Solutions should address changing organizational models as well as economic factors. In response, some companies are developing in-house training programs. Other organizations are examining the impact of outsourced models on CRA performance as well as their onboarding processes and training programs to implement crucial changes to current practices.
- Consider experiential training approaches based on spiral learning that may prepare CRAs to perform effectively without two years’ experience.
- The aviation industry trains pilots using simulation, scenarios, and real-time coaching by expert pilots and may be a useful model from which we can learn when designing curricula for training and preparing CRAs to actually monitor clinical trials in the field.
Mary Jo Lamberti, PhD, associate director and research assistant professor, Abigail Dirks, research data analyst, Robert Howie, advisory committee member, and Ken Getz, executive director and research professor; all with Tufts CSDD
References
- Hill M. Clinical research sites share cash and workforce shortage concerns. Clinical Leader. Published online July 21, 2022.Available at: https://www.clinicalleader.com/doc/clinical-research-sites-share-cash-workforce-shortage-concerns-0001
- Wieland A. What is really behind the CRA shortage in clinical trials? A root causes analysis. Published online May 18, 2020. Available at: https://www.clinicalleader.com/doc/what-s-really-behind-the-cra-shortage-in-clinical-trials-a-root-cause-analysis-0001
- Sonstein S, Samuels E, Aldinger C et al. Self-assessed competencies of clinical research professionals and recommendations for further education and training. Therapeutic Innovation and Regulatory Science. 2022; 56:607-615. Published online March 31, 2022. doi: 10.1007/s43441-022-00395-z. Available at: https://rdcu.be/cY9OR
- Sonstein S, Silva H, Thomas-Jones C et al. Global self-assessment of competencies, role relevance, and training needs among clinical research professionals. Clinical Res. 2016;30(6):42-9. Available at: https://acrpnet.org/2016/12/01/global-self-assessment-of-competencies/
- Barriers to Bridges: Addressing the Urgent Need for a Diverse, Research-Ready Workforce within the Clinical research profession. ACRP Whitepaper. September 2022 p. 7. Available at: https://acrpnet.org/barriers-to-bridges-addressing-the-urgent-need-for-a-diverse-research-ready-workforce-within-the-clinical-research-profession/
- Alsumidae M. Entry-level CRA shortage still crippling trials. Applied Clinical Trials. Published online March 2, 2022. Available at: https://www.appliedclinicaltrialsonline.com/view/entry-level-cra-shortage-still-crippling-clinical-trials
- Alsumidae M. CRA Skills Lack in Critical Areas. Applied Clinical Trials. Published online May 22, 2018. Available at: https://www.appliedclinicaltrialsonline.com/view/cra-skills-lacking-critical-areas
- Survey conducted by Connelly Partners Health for Virb, Inc., March 2022.



Разрешение на строительство — это государственный запись, выписываемый управомоченными учреждениями государственного аппарата или местного управления, который допускает начать строительную деятельность или исполнение строительных операций.
Порядок получения разрешения на строительство устанавливает юридические положения и требования к строительному процессу, включая предусмотренные виды работ, допустимые материалы и подходы, а также включает строительные нормы и комплексы защиты. Получение разрешения на строительные работы является обязательным документов для строительной сферы.
https://tv-master63.ru
Быстромонтируемые строения – это актуальные конструкции, которые отличаются высокой быстротой установки и мобильностью. Они представляют собой сооруженные объекты, состоящие из предварительно созданных элементов или же модулей, которые способны быть скоро смонтированы на участке застройки.
Строительство зданий из сэндвич панелей располагают податливостью также адаптируемостью, что позволяет легко преобразовывать и переделывать их в соответствии с потребностями покупателя. Это экономически выгодное а также экологически стойкое решение, которое в крайние лета заполучило обширное распространение.
After study a couple of of the blog posts on your web site now, and I really like your method of blogging. I bookmarked it to my bookmark website list and will likely be checking again soon. Pls try my website as well and let me know what you think.
Hi there! I just wish to offer you a huge thumbs up for your great information you have here on this post.
I will be coming back to your site for more soon.
It’s remarkable to go to see this web site and reading the views
of all friends regarding this post, while I am also keen of getting
knowledge.
prinivil drug cost
zoloft ocd
buy retin a 1
albuterol brand name usa
proventil inhaler for sale
sildenafil 85
propranolol brand india
Do you have a spam issue on this website; I also am a blogger, and I was curious about your situation; we have created some nice practices and we are looking to exchange solutions with others, be sure to shoot me an e-mail if interested.
synthroid tablets 75 mcg
20mg fluoxetine
furosemide 3170
how to get toradol
diflucan otc where to buy
phenergan tablet cost
budesonide 3 mg capsule cost
I’m very happy to read this. This is the kind of manual that needs to be given and not the random misinformation that is at the other blogs. Appreciate your sharing this best doc.
trazodone 5 mg
combivent 18 103 mcg
fildena 50
neurontin cap 300mg
buy gabapentin 600 mg online
neurontin price india
lisinopril 20 mg canadian
how much is generic synthroid
vurcazkircazpatliycaz.uSSp6vfVAxAm
prinivil lisinopril
phenergan 25g
daktilogibigibi.zrqDThplilL4
Hi there! This post couldn’t be written any better! Reading through this post reminds me of my previous room mate! He always kept talking about this. I will forward this article to him. Pretty sure he will have a good read. Thank you for sharing!
tadalafil 2.5
hydroxychloroquine
fildena 120
tsmavic.wordpress.com – самые сильные привороты по фото
заговор на любовь мужчины на расстоянии читать быстродействующий на растущую луну, вызвать любимого к себе заговор быстродействующий
http://www.magecam.ru – самый сильный рунический приворотный став
Возможны ли нормальные отношения с женщиной Манипуляция людьми —
что с ней делать в отношениях МЕТОДЫ ПОЗИТИВНОЙ ПСИХОЛОГИИ 10 черт человека, который себя не уважает, а
другие этим пользуются
Чеклист: 7 признаков, что люди вами пользуются
synthroid 137 mcg cost
xyandanxvurulmus.0h1QalSPeDM2
xbunedirloooo.D2Q13CrzxBp2
robaxin gold
nominativally xyandanxvurulmus.t2SfoUFkakJZ
Good morning!
Have you ever heard of X-GPT Writer: a unique keyword content generator based on the ChatGPT neural network?
I also haven’t, until I was advised to automate routine tasks with this software, I want to say one thing! For a long time afterwards, I couldn’t believe
that ChatGPT was such a powerful product if it was used simultaneously in streaming, running X-GPT Writer.
I thought it was just a utility, it was inexpensive, a friend gave me a coupon for a 40% discount%:
94EB516BCF484B27
the details of where to enter it are indicated on the website:
https://www.xtranslator.ru/x-gpt-writer/
I started trying, delving into it, bought 50 ChatGPT accounts at low prices and off I went!
Now I easily generate and launch 3-4 new sites per week, batch unify entire folders and even create images
using the ChatGPT neural network and X-GPT Writer.
It’s worth a try, Friends, there’s a demo, everything is free, you won’t regret it)
Good luck!
Генерация текстовых материалов с X-GPTWriter
ChatGPT и создание качественного контента
Эффективное использование ChatGPT для контент-стратегии
Создание контента с помощью X-GPTWriter
Уникализация контента с ChatGPT и X-GPTWriter
ChatGPT для профессиональных копирайтеров и маркетологов
ChatGPT и его роль в создании уникального контента
ChatGPT для уникального исходного контента
Секреты создания контента с ChatGPT
Преимущества использования X-GPTWriter для SEO
tradeswoman xyandanxvurulmus.AnFb9uxRA9W8
where to buy super avana in so ca
cheap amoxicillin tablets
where to buy tadalafil 20mg
accutane cost australia
where can i get trazodone
очень сильные черные привороты – Обратится к магу – dzen.ru/id/653538d7d6100f7a6fee8469
приворот и черная магия
augmentin online canada
cheap accutane online
Проведение сильных любовных приворотов по фотографии.
Обратиться к магу за приворото, почитать отзывы mirprivorotov.ru.
снять черный приворот
can you purchase tadalafil in the us
how does tadalafil work
generic zestoretic
tretinoin 0.04 gel coupon
Hey! I could have sworn I’ve been to this website before but after checking through some of the post I realized it’s new to me. Anyhow, I’m definitely glad I found it and I’ll be bookmarking and checking back often!
отзывы приворота на воду – почитать отзывы о привороте
отзывы на кладбищенские привороты
price of zoloft 50 mg
sildenafil 50 mg tablet
You are my inspiration , I have few blogs and very sporadically run out from to post .
where can i buy vermox medication online
amoxicillin tablet
inderal cost canada
Какие виды потребностей свойственны практически всем людям.
Человек и люди в чем разница. Иррациональный значение. Ответ организма на какой либо раздражитель в психологии ощущений называется. Тест на проверку психики.
Какие основные отличительные признаки
характеризуют человека как соц
существо. Мбии. Чувствительное восприятие это.
where to buy vardenafil
augmentin 500 mg discount
effexor xr 75
Каким цветом инь. Если человек
выбирает синий цвет. Как мыслить критически. Мотивационные фильмы для детей. Поздравление с днем рождения галине красивые
открытки. Сочинение на тему все люди
личности обществознание 6 класс кратко.
От какого цвета отдыхают глаза.
Мбти тест 16.
buy cheap amoxicillin uk
can i buy diflucan over the counter in australia
how to get accutane in india
generic tadalafil cost
fildena 100 free shipping
gabapentin 6
effexor tablets
price of metformin in canada
tadalafil 20 mg canada
discount trazodone
sildenafil nz buy
Последний вечер соловьевым. Вечер с соловьевым воскресный последний. Смотреть соловьева последний
выпуск. Соловьев воскресный вечер последний выпуск.
Вечер с владимиром соловьевым смотреть онлайн прямой эфир.
gabapentin 300mg cost
tadalafil is not for consumption in united states
ivermectin pill cost
Когда речь заходит о микрозаймах, невозможно переоценить значимость надежной информации. На mikro-zaim-online.ru наша команда, в лице таких специалистов как Андрей Фролов и Екатерина Подольская, берет на себя ответственность предоставлять только проверенные данные. Андрей, с его обширными знаниями в банковском деле, и Екатерина, гарантирующая непрерывную и безопасную работу сайта, выбирают для вас только те МФО, которые состоят в реестре ЦБ РФ и работают прозрачно. Подробнее на https://mikro-zaim-online.ru/o-nas/
zhengzhou debao tadalafil
semaglutide 7 mg tablet
wegovy 3 mg
Возник вопрос отправить деньги в черногорию ? На denezhnye-perevody-iz-rossii.top вы найдете легкий способ осуществления международных денежных операций. Мы предлагаем выгодные условия и гарантию безопасности каждой транзакции. Наш сервис позволяет отправлять деньги из Австралии в любую точку мира с минимальными комиссиями и максимальным удобством. Заходите на наш сайт и убедитесь в преимуществах работы с профессионалами.
bactrim d5
Ты знаешь, как бывает: идешь мимо магазина, видишь идеальные кроссовки, но зелени нет. Вспомнил про mikro-zaim-online.ru, решил взять займ на карту. Буквально за 5 минут деньги у меня, и я уже с новыми кроссами. Как говорится, стиль не ждет!
MIKRO-ZAIM – микрозайм
Наши контакты: Зеленодольская улица, 36к2, Москва, 109457
flagyl vial
Когда мой автомобиль внезапно вышел из строя, а ремонт обещал быть дорогостоящим, я нашел выход на mikro-zaim-online.ru. Займ в 10 000 рублей помог мне быстро справиться с проблемой, не оставляя машину в гараже на неопределенный срок. Таким образом, я сэкономил время и нервы, быстро вернувшись на дорогу.
MIKRO-ZAIM – займ быстрый на карту
Наши контакты: Зеленодольская улица, 36к2, Москва, 109457
Планируете денежный перевод из сингапура в россию в 2024 ? Выбор denezhnye-perevody-iz-rossii.top для этой задачи – рациональное решение. Сервис предлагает превосходное соотношение цены и качества, обеспечивая высокую скорость перевода при минимальных комиссиях. Кроме того, важно подчеркнуть преимущество полной безопасности транзакции благодаря современным технологиям шифрования.
wegovy sale
buy wegovy online no script needed
Сделать как перевести деньги из сша просто, если знаешь, куда обратиться. На denezhnye-perevody-iz-rossii.top ты найдешь удобные способы перевода денег из Греции с минимальными комиссиями. Мы обеспечиваем безопасность твоих средств, используя передовые технологии. Помни, что правильный выбор платформы для переводов – это залог успешной финансовой операции.
Выдающийся финансист нового поколения, Андрей Фролов, начал свой путь с блестящего окончания МГУ, затем добился значительных успехов в банковской сфере. Его уникальный подход к решению финансовых задач и мастерство в анализе рынка теперь служат основой для работы сайта mikro-zaim-online.ru. Андрей предлагает клиентам наилучшие условия микрозаймов. Больше информации о его работе и микрозаймах доступно на https://mikro-zaim-online.ru/o-nas/
order wegovy
semaglutide oral medication
Моя девушка переходила на новую должность, и я хотел подарить ей нечто, что поможет ей в работе. Я взял займ через сервис и приобрел ей мощный телефон, который стал надежным помощником в ее профессиональной деятельности.
rybelsus pill
Мой рыболовный снаряжение нуждалось в серьезном обновлении, и я не мог себе позволить упустить начало рыболовного сезона. С помощью сервиса я взял займ и обновил все необходимое для удачной рыбалки.
Мой рыболовный снаряжение нуждалось в серьезном обновлении, и я не мог себе позволить упустить начало рыболовного сезона. С помощью сервиса я взял займ и обновил все необходимое для удачной рыбалки.
Моя попугайчик заболел, и мне срочно нужны были деньги на консультацию у ветеринара. Спасибо постабанку, я получил необходимый займ и помог своему пернатому другу выздороветь.
В любое время суток, когда вам срочно потребуются денежные средства, expl0it.ru предлагает решение: займ онлайн круглосуточно без отказа. Это уникальная возможность получить финансовую помощь, не зависящую от времени дня и без риска отказа. Мы понимаем важность быстрого реагирования на ваши финансовые потребности и предлагаем простую и удобную систему оформления займов, доступную вам 24/7. Ваша финансовая свобода начинается здесь и сейчас!
rybelsus over the counter
Если вам срочно нужны финансы, то expl0it.ru – это то место, где вы можете легко получить займы онлайн. Здесь вы найдете самые выгодные предложения от МФО, которые готовы быстро выдать необходимую сумму на выгодных условиях. Простота и удобство получения займа сделают ваш финансовый опыт максимально приятным.
I just like the valuable info you supply for your articles. I’ll bookmark your blog and check once more right here frequently. I am relatively certain I’ll be informed plenty of new stuff proper right here! Good luck for the next!
Если вам срочно нужны финансы, то expl0it.ru – это то место, где вы можете легко получить займы онлайн. Здесь вы найдете самые выгодные предложения от МФО, которые готовы быстро выдать необходимую сумму на выгодных условиях. Простота и удобство получения займа сделают ваш финансовый опыт максимально приятным.
semaglutide xr
semaglutide online order
rybelsus online cheap
digiapk.com
믿을 수 없었지만 사실은… 실패하더라도 받아들일 수 있었다.
semaglutide generic cost
digiapk.com
장 황후는 몸을 앞으로 숙이고 비단 부두 옆에 앉았습니다. “폐하, 서두르지 않으십니까?”
В мире, где каждую минуту что-то меняется, важно знать, что вы можете положиться на быструю финансовую помощь. Expl0it.ru предлагает вам уникальную возможность получить займ на карту без отказа, что является реальным спасением в непредвиденных обстоятельствах. Забудьте о стрессе и долгих ожиданиях! Здесь вы обретете не только необходимые средства, но и уверенность в завтрашнем дне. Ваша финансовая стабильность начинается с одного клика на expl0it.ru.
where can i buy semaglutide
buy wegovy
ozempic tablets for weight loss
semaglutide retail price
rybelsus tablets cost
saungsantoso.com
남자들은 괜찮지만 여자 친척들은 할 일이 없습니다.
order wegovy
rybelsus
Все мы любим новинки в мире игр, но часто сталкиваемся с трудностями при их поиске. Сайт игры новинки скачать торрент призван решить эту проблему раз и навсегда. Забудь о долгих часах в ожидании загрузки и ненадежных источниках. Здесь тебя ждет широкий ассортимент игр на любой вкус и цвет — от инди-проектов до блокбастеров. Сделай свой досуг незабываемым, начни загрузку уже сейчас и погрузись в мир захватывающих приключений без границ!
Your article was indeed entertaining. I look forward to further agreeable contributions from you. However, how might we communicate?
Как насчет того, чтобы забежать в будущее и посмотреть, что тебя ждет в мире игр? Сайт, где можно скачать торрент игры 2024 на пк, откроет двери в грядущий год, наполненный новыми возможностями и невиданными мирами. Здесь ты найдешь игры, которые только начинают набирать популярность, и ты можешь стать одним из первопроходцев, исследующих их. Не упусти свой шанс быть в авангарде игровой индустрии. Вперед, в будущее, где каждая игра – это новая глава в книге твоих приключений!
wegovy semaglutide
Елена хотела сделать сюрприз и купить дорогой подарок мужу на годовщину, но зарплата задерживалась. После чтения советов в статье на Яндекс Дзен, она нашла надежное МФО, где смогла мгновенно получить необходимую сумму на выгодных условиях, и подарок был куплен вовремя.
DZEN Spavkin – займ до зарплаты на карту
wegovy 21 mg
Дмитрий хотел пройти курс повышения квалификации стоимостью 15 000 рублей. Он воспользовался информацией из статьи и получил займ, несмотря на свою плохую кредитную историю, что позволило ему поднять свои профессиональные навыки на новый уровень.
DZEN Spavkin – все займы онлайн на карту
homefronttoheartland.com
그래서 그녀는 재빨리 응답했고 즉시 몇 명의 메이드를 데리고 패스트리를 만들었습니다.
semaglutide online order
semaglutide 7 mg tablet
semaglutide pill
В жизни каждого бывают моменты, когда средства требуются немедленно. Сайт mikro-zaim-online.ru предоставляет возможность быстро решить финансовые проблемы, предлагая онлайн займы на карту без отказа. Благодаря этому предложению, вы можете быть уверены в том, что получите необходимую сумму в кратчайшие сроки, без лишних задержек и проверок.
Наш сайт mikro-zaim-online.ru – это место, где вы найдете МФО, которые действительно готовы выдать займы каждому, даже если у вас нет официального дохода. Мы специализируемся на подборе финансовых решений, обеспечивающих доступ к займам всем без отказа на карту, независимо от финансовой ситуации. Это означает, что вы можете рассчитывать на нашу помощь, если вам срочно нужны деньги, но нет официального дохода. Мы гарантируем, что каждый заемщик будет обслужен без лишних ограничений и проверок, обеспечивая быстрое и удобное получение финансовой помощи.
wegovy mexico
buy semaglutide
tsrrub.com
이에 비해 단순한 유리와 온실은 약간의 이익만 제공합니다.
semaglutide xr
digiyumi.com
창을 손에 들고 동료들이 모두 주변에 있었기 때문에 그는 그다지 긴장하지 않았습니다.
generic ozempic for weight loss
Доброго!
Было ли у вас опыт написания диплома в сжатые сроки? Это действительно сложное и ответственное занятие, но важно не унывать и продолжать двигаться вперед, уделяя внимание учебным процессам, в которых я также активно участвую.
Для тех, кто умеет быстро находить нужную информацию в интернете, это действительно ценный навык. Это позволяет сократить время на поиск материалов в библиотеках или на встречи с научными руководителями. Если вам требуются хорошие данные для подготовки дипломной работы или курсовых проектов, я могу поделиться полезными ссылками.
http://vuzdiploma.ru/
Желаю всем отличных оценок!
купить диплом в чапаевске
купить диплом в орске
купить диплом в рубцовске
купить дипломы о высшем цены
купить диплом в балашихе
купить диплом в кисловодске
купить диплом в йошкар-оле
куплю диплом высшего образования
купить диплом ссср
купить диплом зубного техника
buy rybelsus from canada
ozempic tablets
Не упустите шанс воспользоваться выгодными предложениями от all-credit.ru – портала, который собрал лучшие займы онлайн. У нас вы получите полную прозрачность сделок, информацию без предвзятости и поддержку на каждом шагу выбора и оформления займа. Воспользуйтесь нашими услугами, и убедитесь, что финансы могут быть простыми и доступными каждому!
brand ozempic
agonaga.com
Liu Jian과 다른 사람들도 안도한 듯 몸을 숙이고 앉았다.
Здравствуйте!
Было ли у вас опыт написания диплома в сжатые сроки? Это действительно сложное и ответственное занятие, но важно не унывать и продолжать двигаться вперед, уделяя внимание учебным процессам, в которых я также активно участвую.
Для тех, кто умеет быстро находить нужную информацию в интернете, это действительно ценный навык. Это позволяет сократить время на поиск материалов в библиотеках или на встречи с научными руководителями. Если вам требуются хорошие данные для подготовки дипломной работы или курсовых проектов, я могу поделиться полезными ссылками.
http://vuzdiploma.ru/
Желаю всем отличных оценок!
купить диплом в магадане
купить диплом сантехника
купить диплом продавца
купить диплом в донском
купить диплом инженера строителя
купить диплом о среднем
купить диплом в озёрске
купить диплом в горно-алтайске
купить диплом лаборанта
купить диплом бурильщика
Представьте место, где каждый визит — это путешествие в мир комфорта и гармонии. termburg.ru вас приветствует, открывая двери в свои уникальные пространства, где можно забыть о времени и насладиться мгновениями чистого счастья. Здесь каждый найдет что-то особенное: будь то умиротворяющая прохлада термального бассейна или теплые объятия травяной сауны. Подарите себе возможность пережить эти моменты, посетив наш сайт termburg.ru. Ваше приключение в мир релакса и удовольствия начинается с одного клика.
ТЕРМБУРГ – термальный комплекс термбург
Адрес – Москва, Гурьянова 30 (2 этаж)
wegovy tab 3mg
ozempic
this-is-a-small-world.com
Zhu Houzhao는 밤낮으로 그것을 기대했지만 누군가 반항했습니다.
semaglutide online uk
semaglutide coupon
wegovy 3 mg
natural metformin
ozempic semaglutide tablets cost
binsunvipp.com
그러나 Zhang Yanling은 “형제님, 무슨 일이세요, 무슨 일이세요. “라고 말했습니다.
wegovy semaglutide tablets cost
rybelsus best price
rybelsus 7 mg tablet
rybelsus australia online
ozempic semaglutide
buy semaglutide cheap
Сталкиваетесь с неожиданными финансовыми трудностями? На нашем сайте вы найдете мфо без отказа на карту круглосуточно без проверок, предлагающие быстрые займы с гарантией одобрения и без необходимости предоставления справок.
Heya i am for the first time here. I found this board and I find It truly
useful & it helped me out a lot. I hope to give something back and aid others like you
helped me.
This paragraph offers clear idea in favor of
the new people of blogging, that actually how to do running a blog.
netovideo.com
거의 모든 사람들이 Beizhen Fusi의 이 보고서를 주의 깊게 듣고 있습니다.
Вы ищете финансовую поддержку, но не знаете, куда обратиться? Посетите наш сайт, где мы собрали информацию о мфо малоизвестные, предлагающие удобные и выгодные условия для быстрого получения денег. Откройте для себя новые возможности без лишних хлопот и с дружелюбным сервисом.
Пройдите курсы повышения квалификации для педагогов в Академии “МАПС” и откройте новые перспективы в вашей профессиональной карьере. Наши дистанционные программы позволяют обновить знания и приобрести новые навыки, не выходя из дома. Развивайтесь вместе с нами, чтобы вдохновлять своих учеников на новые достижения каждый день.
Maps-Edu – аккредитация биологов
I was curious if you ever thought of changing the page layout of your website?
Its very well written; I love what youve got to say. But maybe you could a little more in the way of
content so people could connect with it better.
Youve got an awful lot of text for only having one or two images.
Maybe you could space it out better?
rybelsus 3 mg
yangsfitness.com
빚이 얽히고, 세금은 날로 늘어나지만 지출도 늘어나고 있다.
Nice post. I learn something new and challenging on sites I stumbleupon every day.
It will always be helpful to read content from other writers and use something from other
websites.
Hi everyone, it’s my first go to see at this web site, and post is really fruitful
in support of me, keep up posting these types of posts.
Получите вашу аккредитацию медицинских работников вместе с Академией “МАПС”! Профессиональное развитие и подтверждение квалификации теперь доступны из любой точки России. Наша программа обучения обеспечивает все необходимые знания и навыки для успешного прохождения аккредитации. Присоединяйтесь к числу квалифицированных специалистов уже сегодня!
Maps-Edu – курсы сиделок
semaglutide 14mg
Great delivery. Great arguments. Keep up the good spirit.
I think this is one of the most important info for me. And i am glad reading your article.
But want to remark on some general things, The site style is wonderful,
the articles is really nice : D. Good job, cheers
Не знаете, где найти надежный займ? Исследуйте нашу коллекцию мфо займы, где каждый сможет найти что-то подходящее для себя. Независимо от вашей кредитной истории или финансового положения, у нас есть предложения, которые помогут вам в трудной ситуации.
Pretty! This was an extremely wonderful article.
Thanks for providing this information.
Пройдите курсы повышения квалификации для педагогов в Академии “МАПС” и откройте новые перспективы в вашей профессиональной карьере. Наши дистанционные программы позволяют обновить знания и приобрести новые навыки, не выходя из дома. Развивайтесь вместе с нами, чтобы вдохновлять своих учеников на новые достижения каждый день.
Maps-Edu – профессиональная переподготовка для врачей
rybelsus 14mg tablets
semaglutide cost
Very quickly this web site will be famous among all blogging
visitors, due to it’s nice articles
Hello, this weekend is pleasant for me, for the
reason that this time i am reading this fantastic educational piece of writing here at my house.
Magnificent beat ! I would like to apprentice at the same time as
you amend your web site, how can i subscribe for a
weblog website? The account helped me a appropriate deal.
I had been tiny bit acquainted of this your broadcast offered shiny clear concept
What’s Going down i’m new to this, I stumbled upon this I have found It
positively helpful and it has helped me out loads. I am hoping to contribute & aid different
users like its helped me. Great job.
where can i buy furosemide
wegovy diabetes medication
generic lisinopril
dota2answers.com
이것이 Fang Jifan이 Zhou Tangsheng을 보내러 온 이유이기도 합니다.
zoloft migraine
buy semaglutide from canada online
rybelsus australia
lasix for hyperkalemia
gabapentin side effects in cats
Я давно занимаюсь разработкой программного обеспечения и мне срочно потребовался апгрейд моего рабочего компьютера для выполнения нового крупного проекта. Мне необходимо было установить дополнительную оперативную память и мощный процессор, чтобы обеспечить необходимую производительность. Хотя моя кредитная история была безупречной, я предпочитал не тратить время на длительные банковские процедуры. Мне требовалось быстро найти 25 000 рублей. Я решил воспользоваться услугами МФО 2024 года, которые предлагают быстрые займы под удобные проценты. Благодаря этому я смог немедленно приобрести необходимые комплектующие и успешно приступить к реализации проекта.
Находясь в поиске быстрого решения финансовых вопросов без отказа, я наткнулся на отличный ресурс. Рекомендую всем, кто находится в сложной ситуации, перейти по займ без отказа в новых МФО. Здесь вы найдете проверенные МФО 2024 года, готовые оказать помощь без предвзятости к вашей кредитной истории.
glucophage maigrire
side effects of zithromax
cephalexin tooth infection
yangsfitness.com
상대가 방향타를 돌릴 기미가 거의 없었다.
is gabapentin used for anxiety
wegovy rx
Если Вы хотели найти дизайн интерьера дома в сети интернет, то Вы на нужном пути. Звоните по телефону +7(812)408-00-07 или пишите на нашем сайте. Студия расположена по адресу: г. Санкт-Петербург, ул. Мебельная, д. 49/92. Режим работы по будням с 9:00 до 19:00. Наши консультанты дадут ответы на любые оставшиеся вопросы, дадут советы по вашему проекту и в быстром времени подойдут к оформлению договора и будущей работе.
Дизайн СПБ mudryakova.ru
amoxicillin dosage pediatric
Для того, чтобы ваша бытовая техника Indesit служила вам долго и без сбоев, вам нужен опытный и квалифицированный сервисный центр, такой как indesit-ekaterinburg.ru. Мы гарантируем, что после ремонта в нашем сервисном центре ваша техника Indesit будет работать как новая, так как мы выполняем все виды работ, от диагностики до замены деталей. Мы ценим наших клиентов и делаем все, чтобы они оставались довольны нашей работой. Поэтому мы предоставляем бесплатную консультацию, гибкий график работы и гарантию на все виды ремонта.
order semaglutide online
Если Вы искали дизайн интерьера в сети интернет, то Вы на правильном пути. Звоните по номеру телефона +7(812)408-00-07 или пишите на нашем сайте. Студия находится по адресу: г. Санкт-Петербург, ул. Мебельная, д. 49/92. Режим работы по будням с 9:00 до 19:00. Наши дизайнеры дадут ответы на любые оставшиеся вопросы, дадут рекомендации по вашему проекту и в быстром времени перейдут к заключению договора и будущей работе.
Дизайн квартиры под ключ mudryakova.ru
pragmatic-ko.com
수백 척의 배가 갑자기 부풀어 오르기 시작했습니다.
cephalexin for strep
По запросу услуги дизайнера заходите на наш онлайн ресурс. Работаем с определенно разными проектами, как под ключ, так и с едиными небольшими комнатами. Начинаем работу, естественно, со общения с вами, ведь каждый интерьер создается под собственника квартиры, целую семью или владельца отеля. У каждого человека свои потребности, задачи помещения, образы жизни и нравы, а также мечты и требования. Мы пытаемся учесть все мелочи и соединить их в особенном дизайн проект.
Портфолио дизайна интерьера mudryakova.ru
Я был приятно удивлен качеством и скоростью ремонта в сервисном центре service4lenovo.ru. Они восстановили мои данные и настроили мой компьютер Lenovo, а также дали мне гарантийный талон на скидку 10% на следующий ремонт. Я был в восторге от их профессионализма и внимания к клиенту, а также от того, что они работают круглосуточно и без выходных.
order ozempic
ciprofloxacin and amoxicillin
rybelsus online uk
pragmatic-ko.com
Fang Jifan의 방법에 따라 방향을 360도로 직접 나누었습니다.그들 자신은 군사적 문해력이 전혀 없으며 현재 완전히 무너졌습니다.
jbustinphoto.com
그의 전하만이 여전히 멍해 보였다.
ozempic tab 7mg
rybelsus mexico
buy rybelsus from canada
По теме детские солнцезащитные очки купить мы Вам обязательно поможем. Очки — объект, который эксплуатируют почти все. Летом это необходимый атрибут, который защищает глаза от вредоносного УФ излучения. Вот вот уже скоро наступит летняя пора и не забудьте заблаговременно позаботиться и осчастливить себя классным и необходимым атрибутом. Помимо того, очки — это отличный подарок для всякого человека, любого возраста и пола..
pragmatic-ko.com
이것은 포격의 시험사격으로 매우 위력이 높았으나 인명피해는 많지 않았다.
wegovy 7 mg tablet
dosage of bactrim for sinus infection
switching from amoxicillin to cephalexin
Спасибо за информацию. В благодарность предлагаю расслабиться и окунуться в мир азарта:
официальный сайт Вавада – это крутой метод, позволяющий вам окунуться в мир азартных игр в одном из лучших онлайн-казино. Для начала, откройте официальный сайт Vavada и нажмите на кнопку “Регистрация”. Затем заполните простую форму регистрации своими личными данными.После успешной регистрации вы получите доступ к широкому выбору азартных игр, таких как слоты, рулетка, блэкджек и многое другое. Казино Вавада также щедро раздрает бонусы, которые значительно повышают вероятность выигрыша. Играйте с умом и делайте ставки с лимитами. Регистрация в казино Vavada – это крутой метод насладиться азартными играми, получить удовольствие и, вероятно, выиграть хорошие деньги.
pragmatic-ko.com
그 불길은… 흐릿한 하늘 전체를 순식간에 비췄다.
Hi i think that i saw you visited my web site thus i came to Return the favore Im attempting to find things to enhance my siteI suppose its ok to use a few of your ideas
[url=http://rybelsustabs.shop/]rybelsus tab 14mg[/url]
otc lisinopril
По поводу душевой уголок 120×90 заходите на указанный веб сайт. В данное современное время дизайнеры и даже сами обладатели дома делают из простых помещений красивейшие произведения искусства и максимально уютные условия. Ванная комната не является исключением, из них получаются шикарные интерьеры с наличием ванны, унитаза и раковин. У нас в каталоге Вы найдете: ванны, душевые кабины, шторки на ванну, двери в нишу, трапы, писсуары, системы инсталляции, раковины, смесители, светильники, аксессуары и многое другое
mikschai.com
Zhu Hou는 Fang Jifan의 신중한 생각을 통해 보는 미덕으로 Fang Jifan을 돌 보았습니다.
twichclip.com
게으름을 생각하며 Zhu Houzhao는 눈을 들어 맞은편에서 행복하게 식사를 하고 있는 Fang Jifan을 보았다.
I have been examinating out a few of your articles and it’s pretty good stuff. I will definitely bookmark your site.
synthroid 112 mcg tab
gabapentin 300mg dosage
hihouse420.com
아니나 다를까, 좋은 형제는 헛되지 않으며, 중요한 순간에 항상 나타날 수 있습니다.
Hi my friend! I wish to say that this article is awesome, nice written and include almost all important infos. I’d like to see more posts like this.
can you buy azithromycin over the counter in australia
lisinopril 25 mg price
how to buy metformin in usa
tadalafil canada price
Проверенные букмекерские конторы
Относительно зеркало бк марафон вы сможете найти всё о ставках на спорт, бонусы новым игрокам и детальные прогнозы. Так как ставки на спорт основные сайты букмекерских контор регулярно блокируют, то разрабатываются рабочие сайты — зеркала. У нас Вы можете войти в такие бк, как мостбет, марафонбет, melbet, 1 икс бет и другие. Только самые известные и проверенные компании, за которые не нужно переживать.
apksuccess.com
지금 이 순간 그들이 진정으로 그리워하는 것은 가족이다.
Вход в БК
Относительно вход на официальный сайт 1xbet вы сможете найти всё о ставках на спорт, подарки новым игрокам и детальные прогнозы. Так как ставки на спорт официальные сайты БК постоянно банят, то делаются рабочие площадки — зеркала. У нас Вы можете войти в такие конторы, как мостбет, марафонбет, melbet, 1xbet и другие. Только самые популярные и проверенные конторы, за которые не нужно волноваться.
Предприниматели и бизнес-руководители, стремящиеся к надежности и юридической защите, найдут оптимальное решение в нашей услуге юридическое абонентское обслуживание. Это не просто услуга, это ваш юридический щит от всех неожиданностей. Наша команда профессионалов гарантирует круглосуточную поддержку, предотвращение юридических рисков и оптимизацию вашего бизнеса. Переходите на svoyuristonline.ru и обезопасьте свое предприятие от юридических неприятностей уже сегодня.
synthroid lowest prices
Малый бизнес требует тщательного внимания и профессионального юридического подхода. Обратившись к нам, вы получите юридическое сопровождение малого бизнеса, которое поможет избежать многих типичных ошибок и защитит вас от непредвиденных юридических рисков. Наши услуги включают полный спектр юридической поддержки, от договорной работы до представления интересов в судах. Защитите свой бизнес уже сегодня, посетив svoyuristonline.ru
Забота о юридической безопасности вашего бизнеса – наш приоритет. С услугой юридическая защита бизнеса, предлагаемой нашей компанией, вы получаете гарантию комплексного подхода к защите ваших прав и интересов. Предупреждение юридических угроз, консультации и сопровождение сделок – всё это доступно на svoyuristonline.ru
Зеркало БК действующее на сегодня
Что касается marathonbet вы сможете найти всё о ставках на спорт, бонусы новичкам и прогнозы. Так как ставки на спорт официальные сайты букмекерских контор регулярно банят, то создаются рабочие площадки — зеркала. У нас Вы можете войти в такие конторы, как мостбет, марафонбет, мелбет, 1 икс бет и другие. Только самые популярные и надежные компании, за которые не нужно волноваться.
manzanaresstereo.com
그러나 Tang Yin은 편지에서 몇 가지 우려를 표명했습니다.
generic tadalafil for sale
mega-slot1.com
Liu Jian 세 사람은 눈을 곧게 펴고 어안이 벙벙한 채 서로를 응시하며 무슨 말을 해야 할지 몰랐습니다.
andrejpos.com
그는 왕자와 Fang Jifan과 감히 논쟁하지 않았습니다.
jelenakaludjerovic.com
Zhou 부인은 이미 멀지 않은 구 아슈 가게로 달려갔습니다.
Great post. I was checking constantly this blog and I’m impressed! Very useful info specifically the last part 🙂 I care for such info much. I was looking for this particular info for a long time. Thank you and good luck.
how to buy lisinopril online
Вас приветствует интернет-магазин PUMA Moldova! Ищете стильные и удобные кроссовки? У нас огромный выбор кроссовок PUMA для мужчин и женщин со скидками! Не пропустите уникальную возможность обновить свой спортивный гардероб высококачественной обувью по привлекательным ценам. Помимо кроссовок, у нас вы найдете широкий ассортимент одежды и аксессуаров для всей семьи. Действует бесплатная доставка по Кишиневу. Выбирайте лучшее в PUMA Moldova и наслаждайтесь комфортом и стилем каждый день!
Pumamoldova.md – интернет магазин одежды
Контакты и адрес – Молдова, г. Кишинев
You are my aspiration, I own few blogs and occasionally run out from to post .
depakote davis pdf
strelkaproject.com
이 순간 Xiao Jing의 턱이 거의 떨어졌습니다.
ddavp for enuresis
apksuccess.com
Zhu Houzhao는 서둘러 말했다.
Методы неразрушающего контроля материалов ndt.su
По запросу набор маркировочных знаков цифры Вы попали по нужному адресу. Также рассмотрите наши специальные предложения по акции на настоящий момент: гель для ультразвукового контроля Инспектор, магнитный дефектоскоп на постоянных магнитах, ЭЧК Канавочный эталон чувствительности и другие. Подробный каталог разделен на: капиллярный контроль, ультразвуковой, вакуумный, экзаменационные образцы и другие. Заходите в необходимый Вам класс, отправляйте продукты в заказ или к сравнению с похожими для Вашего точного выбора.
Мы расположены по адресу: РФ, Удмуртская республика, г. Ижевск, ул. Красногвардейская, д. 60, оф. 13. По любому вопросу звоните по контактному телефону 8(800)555-45-19 или пишите на электронную почту. Время работы пн-пт с 9:00 до 18:00, суббота и воскресенье выходные дни.
generic tadalafil 20mg from india
bistroduet.com
그는 여전히 땅에 무릎을 꿇고 있었지만 폐하가 떠났지만 일어나지 못하는 것 같았습니다.
Методы неразрушающего контроля материалов ndt.su
Если Вы желали купить радиографический метод контроля в сети интернет, то перемещайтесь на наш сайт ndt.su уже сейчас. Мы уже много лет работаем в данной сфере и знаем свои продукты превосходно. Также с радостью готовы предложить необходимые продукты определенно для сложившейся ситуации. Мы используем в работе компоненты только Российского происхождения, разумеется нам удается держать цены на уровне, при этом не уступая в качестве. Звоните, заказывайте и Вы не пожалеете.
Мы находимся по адресу: РФ, Удмуртская республика, г. Ижевск, ул. Красногвардейская, д. 60, оф. 13. По любому вопросу звоните по телефону 8(800)555-45-19 или пишите на электронную почту. График работы понедельник-пятница с 9:00 до 18:00, суббота и воскресенье выходные.
purchase cozaar online
metformin 101
Визуальный контроль ndt.su
Если Вы хотели найти вакуумная рамка для контроля герметичности в сети интернет, то перемещайтесь на указанный сайт ndt.su уже сегодня. Мы уже большое количество лет работаем в определенной сфере и знаем свои продукты превосходно. Также с радостью готовы предложить необходимые товары конкретно для вашей ситуации. Мы расходуем в работе детали сугубо Российского происхождения, оттого нам удается держать цены на уровне, при этом не уступая в качестве. Звоните, заказывайте и Вы не пожалеете.
Мы находимся по адресу: РФ, Удмуртская республика, г. Ижевск, ул. Красногвардейская, д. 60, оф. 13. По любому вопросу звоните по телефону 8(800)555-45-19 или пишите на электронный адрес. График работы по будням с 9:00 до 18:00, суббота и воскресенье выходные дни.
synthroid generic
apksuccess.com
그때에는 식량이 부족하여 동물과 사람이 모두 죽을 것입니다.
prednisone uk buy
megabirdsstore.com
Zhu Houzhao는 웃지 않을 수 없었습니다. “당연히 영웅들은 같은 것을 보고 나도 마찬가지입니다.”
depakote side effects
Hi i think that i saw you visited my web site thus i came to Return the favore Im attempting to find things to enhance my siteI suppose its ok to use a few of your ideas
windowsresolution.com
같은 단어를 다른 사람이 말하면 그 효과는 완전히 달라집니다.
metformin 15 mg
what is ddavp
side effects of cozaar generic
metformin 500 mg buy online
lisinopril 40 mg pill
Привет! Хочу поделиться своим приятным опытом. Недавно столкнулся с тем, что неожиданно для меня наступил День Рождения моего друга, а денег на подарок не было. В такие моменты портал zaim-fin.ru становится настоящим спасением! Там я обнаружил много МФО, готовых выдать займы даже людям с плохой кредитной историей. И, самое главное, без лишних заморочек и проверок. Благодаря этому я смог приобрести отличный подарок для друга и устроить ему настоящий праздник! Ещё на этом сайте я нашел много полезной информации о том, как оформить заявку на микрокредит и какие требования у МФО к заемщику. Очень удобно!
hihouse420.com
건강하지 못한 사람은 자신이 다른 사람보다 더 나을 수 있다는 것을 증명하기를 간절히 원합니다.
azithromycin 500 tablet price
synthroid tablets
It’s going to be ending of mine day, except before ending
I am reading this great paragraph to increase my know-how.
shopanho.com
Hongzhi 황제는 즉시 Fang Jifan을 다시보고 “Fang Jifan”이라고 말했습니다.
vasotenal ez simvastatin ezetimibe
diclofenac pill
I carry on listening to the news update lecture about receiving boundless online grant applications so I have been looking around for the best site to get one. Could you advise me please, where could i get some?
Привет, друзья! Сегодня я хочу поделиться с вами своей радостью о том, как портал zaim-fin.ru помог мне создать уютный уголок в моем доме! Давно мечтала обновить интерьер и сделать его более уютным и гармоничным, но финансовые ограничения всегда мешали этому. Но знакомство с zaim-fin.ru принесло свежий вдохновляющий ветер в мою жизнь! Здесь я не только нашла возможность получить займы от различных МФО, но и получила множество идей и советов о том, как создать уютный интерьер, не выходя за пределы бюджета. Благодаря этому ресурсу, я смогла приобрести новую мебель, украсить дом красивыми аксессуарами и создать атмосферу, в которой хочется проводить время! Так что, если у вас есть желание обновить свой дом и создать уютное место для себя и своих близких, обращайтесь к порталу zaim-fin.ru – здесь вас ждут не только финансовые возможности, но и вдохновение для воплощения ваших дизайнерских идей!
Привет, друзья! Когда решаете взять займ, важно знать, как выбрать лучший вариант. Портал zaim-fin.ru поможет вам сделать это. Здесь вы найдете ряд МФО, предоставляющих займы на разные сроки и с разными условиями. Перед выбором займа, обязательно изучите условия предоставления займа, процентные ставки, сроки и скрытые комиссии. Сравните несколько вариантов и выберите тот, который наиболее выгоден и подходит под ваши нужды. Так вы сможете сэкономить на процентах и сделать правильный выбор.
synthroid 75 mg
diltiazem picture
buy zestril
ttbslot.com
Zhu Houzhao는 아버지가 자신에게 묻는 것을 보았을 때 자연스럽게 빨리 말했습니다.
twichclip.com
무서운건… 팡가족… 팡가족… 온가족이 괴물같다.
coming off effexor weight loss
generic flexeril
ttbslot.com
하지만 두 번째가 사실이라면 첫 번째는…
Спасибо за информацию.
Предлагаю вам русские боевики – это невероятное произведение, которое нравится огромному количество зрителей по всему миру. Русские фильмы и сериалы предлагают уникальный взгляд на русскую культуру, историю и обычаи. В настоящее время смотреть русские фильмы и сериалы онлайн стало легко благодаря различным платформам и сервисам. От ужасов до триллеров, от исторических лент до современных детективов – выбор огромен. Окунитесь в захватывающие сюжеты, профессиональную актерскую работу и красивую работу оператора, смотрите фильмы и сериалы из РФ не выходя из дома.
synthroid mcg
flomax time of day to take
Мне бы хотелось поделиться своим положительным опытом с lenovo-remont.com. Данный сервис-центр по-настоящему заслуживает положительного отзыва за высококвалифицированный отношение и качественный ремонт продукции Lenovo.
lisinopril drug
На днях пришлось обратиться в neff-centr.ru чтобы отремонтировать своей духовки Neff. Сервис на высоте – заявку приняли оперативно, специалист был у меня уже на следующий день. Ремонт произвели идеально, с гарантией. Стоимость услуг разумная. Советую обращаться тем, у кого есть техника Neff!
Любители сексуальных наслаждений будут удивлены красотой проституток на сайте newswomanblog.win. Здесь собраны лучшие девушки из сферы интимных услуг, работающие по всей территории Москвы. Они обладают безупречными телами, поэтому способы свести с ума и подарить бесподобные оргазмы. Можно выбрать путану с нужными параметрами: со средней, маленькой или большой грудью; высокую или миниатюрную; с разным цветом волос и типажом. В любом случае она доставит удовольствие и поможет сбросить накопившееся напряжение.
В Москве сейчас не снимешь проститутку у дороги. Зато это можно сделать на сайте newswomanblog.win, где собраны анкеты путан с номерами телефонов и фотографиями. Девушки не будут задавать вопросов и не попросят идти с ними на свидание. Чтобы заняться с ними сексом, достаточно уточнить список услуг и договориться о цене. Можно получить удовольствие на своей территории или приехать в роскошные апартаменты. Минимальное время наедине с проституткой — один час. А если вам этого мало, путана скрасит ваш досуг в течение ночи.
allopurinol and colchicine interaction
aripiprazole drug interactions
qiyezp.com
Fang Jifan은 미소를 지으며 고개를 저었다. “하지만 이곳은 어디에서 왔습니까?”
Не зря говорят, что в Москве проститутки самые красивые и раскрепощенные. Они могут доставить такое наслаждение, которое мужчина никогда не получит в постели с женой ли подругой. Все дело в техниках удовлетворения, которыми путаны владеют в совершенстве. Они без проблем делают горловой минет, позволяют иметь их в попу и т.д. Найти проститутку не сложно — достаточно открыть сайт newswomanblog.win. Здесь размещены анкеты путан, среди которых можно легко выбрать девушку по своим запросам в плане внешности и других параметров.
qiyezp.com
이때 크게 웃는 것은 실로 죽음을 구하는 행위이다.
Не зря говорят, что в Москве проститутки самые красивые и раскрепощенные. Они могут доставить такое наслаждение, которое мужчина никогда не получит в постели с женой ли подругой. Все дело в техниках удовлетворения, которыми путаны владеют в совершенстве. Они без проблем делают горловой минет, позволяют иметь их в попу и т.д. Найти проститутку не сложно — достаточно открыть сайт newswomanblog.win. Здесь размещены анкеты путан, среди которых можно легко выбрать девушку по своим запросам в плане внешности и других параметров.
average cost of zithromax
is tylenol the same as aspirin
Превосходный ремонтный центр servispylesosydajson.ru предоставил мне незабываемый опыт. Команда профессионалов центра быстро и эффективно обнаружили и устранили проблему со моим пылесосом Dyson.
Далее, я был глубоко впечатлен качеством сервиса, предоставленным сервисным центром. Они были очень внимательны ко всем моим потребностям и предоставили ценные рекомендации по уходу за моим пылесосом.
amitriptyline 10mg for sleep
Лучшие советы и ключевые моменты, которые нужно знать перед приобретением квартиры в Истре
Одна из самых важных и сложных решений в жизни – приобретение жилья. В поисках идеального места для проживания мы стремимся найти лучшую комбинацию удобства, комфорта и красоты. Истринский район, с его богатой историей и неповторимой природой, предлагает подобрать вам именно такое место, где можно будет осуществить большую мечту – обрести свой уютный уголок под солнцем.
Локализоваться где-то между северным сиянием и поэтическими пейзажами, Истра приковывает взгляды туристов и покупателей жилья, стремящихся оценить его потенциал. Живописный итог многих картин, на фоне которого вы можете создать свою собственную предысторию. Неважно, ведётся ли речь о семейном накоплении или инвестициях в жилье, Истра – это место, где реальность сливается с мечтой, а возможности кажутся безграничными.
Духом и историческими наследиями пропитанный Истринский район предлагает жилища, полные загадочной атмосферы и радостного ожидания.
Ваша скидка 5% на консультацию с юристом по недвижимости в Истре
sandyterrace.com
이 유니폼 아래에서 그녀는 더욱 영웅적으로 보입니다.
lisinopril 10 mg
В ассортименте нашего интернет-магазина сантехники представлена только оригинальная продукция таких известных брендов как Джилекс, PRO AQUA, Valfex, LD, СТМ и многих других
Если вы столкнулись с необходимостью отремонтировать ваш пылесосу Dyson требуется качественный ремонт и обслуживание, доверьтесь сервисный центр Dyson. Профессионалы быстро выявят причину поломки и устранят проблему, применяя детали от производителя. Подробности о ремонте по ссылке: remontdyson.ru.
baclofen pump picture
donmhomes.com
この記事は本当に目から鱗でした。感謝します。
5mg tadalafil price
buy synthroid canada
augmentin dosage for children
thewiin.com
그 이후로 많은 사람들이 손가락을 꼬집고 계산하기 시작했습니다.
bupropion er
can i buy metformin over the counter in australia
celecoxib dosage for adults
ashwagandha root extract
Электронная регистрация в Росреестре – Сделки онлайн – Центр “Недвижимость и право”
Электронная регистрация в Росреестре сделок с недвижимостью. Ускоренные сроки – 3-7 дней. Выписки из ЕГРН.
Аренда квартир посуточно и на длительный срок, любого типа и комфорта в Крыму и г. Симферополь
prednisone 30 mg price
5mg celexa
naproxen and buspirone
मिशनरी शैली अश्लील qqyyooppxx.p7nAST3tuE5
etsyweddingteam.com
このブログはいつも実用的で価値ある情報を提供してくれます。
बुत अश्लीलता के बा hjkvbasdfzxzz.LsWqvRb0oVa
Обучение управлению государственными и муниципальными закупками предназначено для специалистов, желающих повысить свою квалификацию в области закупочной деятельности. Курс направлен на изучение нормативно-правовой базы, процессов планирования, организации и проведения закупок товаров, работ и услуг для государственных и муниципальных нужд, а также на освоение эффективных стратегий и инструментов в данной сфере.
Развивайте свои навыки: профессиональная переподготовка для логопедов и логопедия переподготовка .
tadalafil online paypal
Курсы повышения квалификации для юристов, доступные через maps-edu.ru, являются важным инструментом для поддержания высокого уровня профессионализма в сфере права. Программы обучения охватывают последние изменения в законодательстве, судебной практике, а также новые тенденции в юриспруденции, обеспечивая юристам необходимые знания и навыки для успешной карьеры и предоставления качественных юридических услуг.
Обновите свои знания: курсы повышения квалификации для педагогов и профессиональная переподготовка юриспруденция дистанционно .
2 synthroid
Чтобы набрать баллы для аккредитации медсестры, необходимо участвовать в различных формах профессионального обучения и развития, включая курсы повышения квалификации, участие в семинарах и конференциях, а также изучение специализированной литературы и прохождение онлайн-курсов. Это позволяет не только набрать необходимое количество баллов, но и поддерживать профессиональный уровень в соответствии с современными требованиями медицины.
Готовьтесь к аккредитации: курсы повышения квалификации для строителей и всесторонняя подготовка для медицинских работников.
Профессиональная переподготовка “Юрист по договорному праву” позволяет специалистам в области права специализироваться на договорных отношениях, которые являются основой большинства коммерческих, финансовых и личных взаимодействий в современном обществе. Курс направлен на изучение актуальных аспектов договорного права, включая составление, анализ, исполнение и расторжение договоров, а также решение споров, связанных с договорными обязательствами.
Освойте новые горизонты: аккредитация медработников и контролю закупок.
एमआईएलए अश्लील txechdyzxca.Hl6TXHBCbZa
qiyezp.com
그는 경멸하는 눈으로 고개를 저으며 “믿을 수 없다”고 말했다.
synthroid 0.112 mg
lisinopril 12.5 mg 10 mg
सेलिब्रिटी अश्लील hkyonet.FoJZoRStkNf
I truly savored what you’ve accomplished here. The sketch is elegant, your authored material trendy, however, you seem to have developed some trepidation about what you aim to offer next. Certainly, I shall revisit more regularly, just as I have been doing nearly all the time, in case you uphold this ascension.
metformin online india
synthroid cheapest prices
tadalafil 10mg generic
qiyezp.com
처음에는 자랑하던 너였지만 지금은 사라진 너야.
Spotlight on Success: 18ps.ru Redefines the Plastic Processing Landscape. In a world where sustainability and efficiency are paramount, 18ps.ru stands out as a trailblazer in the field of plastic processing solutions. With a comprehensive range of equipment tailored to meet the diverse needs of businesses, 18ps.ru is empowering industries to thrive in an ever-changing market. From plastic recycling to granule processing and beyond, 18ps.ru is committed to delivering cutting-edge technology and exceptional service to its customers. Join us as we explore how 18ps.ru is reshaping the industry and setting new standards for excellence in plastic processing.
Eng.18ps.ru – polymer sand equipment
ativan lactose
pbs semaglutide
ladesbet ਮਸ਼ਹੂਰ ਪੋਰਨ ladesinemi.1Clp1aEpqIB
lisinopril 20 mg daily
ladesbet 輪姦ポルノ ladestinemi.OrIlQC7wGES
В https://servisnyjcentr-lenovo.ru/ работают профессионалы, которые смогут отремонтировать любую модель Lenovo. Ваш ноутбук будет как новенький!
сервисный центр леново в москве
заменить корпус ноутбука леново цена
сколько стоит поменять клавиатуру на ноутбуке леново
заменить корпус ноутбука леново
tadalafil for sale online
Разработка товаров в 3D arigami.tech
Если Вы хотели найти мобильное приложение дополненной реальности в интернете, то мы можем Вам помочь. Наше предложение актуально для тематик: дизайн, спорттовары, декор, инструменты, электроника, товары для сада и дачи и другие. Если Вы не можете определиться, что конкретно требуется Вашему бизнесу, то заполните заявку на сайте arigami.tech и наш менеджер Вам перезвонит и даст ответы на все вопросы. Наш контактный номер телефона +7(925)077-93-94 или пишите на вотс ап. Будем рады удачному сотрудничеству с Вами!
acarbose epocrates
Szpiegowskie telefonu – Ukryta aplikacja śledząca, która rejestruje lokalizację, SMS-y, dźwięk rozmów, WhatsApp, Facebook, zdjęcie, kamerę, aktywność w Internecie. Najlepsze do kontroli rodzicielskiej i monitorowania pracowników. Szpiegowskie Telefonu za Darmo – Oprogramowanie Monitorujące Online.
lacolinaecuador.com
내 가정사야, 내 아들아, 풀뿌리일 뿐인 너에게 여기서 헛소리를 하게 놔둬라.
Применение технологий дополненной реальности arigami.tech
Если Вы хотели найти товар 3д в сети интернет, то мы можем Вам оказать помощь. Наше предложение актуально для тематик: ремонт, ретейл, мебель, инструменты, электроника, товары для сада и дачи и другие. Если Вам сложно определиться, что именно требуется Вашему бизнесу, то оформите заявку на сайте arigami.tech и наш консультант Вам перезвонит и даст ответы на все вопросы. Наш контактный номер телефона +7(925)077-93-94 или пишите на вотс ап. Будем рады успешному сотрудничеству с Вами!
Instalación simple y descarga gratuita, no se requieren conocimientos técnicos y no se requiere raíz.Grabacion de llamadas, Grabacion de entorno, Ubicaciones GPS, Mensajes Whatsapp y Facebook, Mensajes SMS y muchas características mas.
abilify reviews
cougarsbkjersey.com
このブログはいつも私の期待を超えてくれます。素晴らしいです!
[url=http://lisinoprilgp.com/]lisinopril cost 40 mg[/url]
Разработка товаров в 3D arigami.tech
Если Вы хотели найти товар в 3д в интернете, то мы можем Вам оказать помощь. Наше предложение подходит для областей: дизайн, спорттовары, декор, оборудование, электроника, товары для сада и дачи и другие. Если Вам сложно понять, что именно требуется Вашему бизнесу, то оформите заявку на сайте arigami.tech и наш консультант Вам перезвонит и даст ответы на возникшие вопросы. Наш контактный номер телефона +7(925)077-93-94 или напишите в телеграм. Будем рады удачному партнерству с Вами!
sandyterrace.com
“할아버지, 이 3,000무의 땅에만 매물이 있다고요?”
Студия разработки виртуальной реальности w2w.group
По запросу разработка приложений дополненной реальности услуги Вы на правильном пути. Наши специалисты готовы дать обратную связь и ответить на возникшие вопросы. Если у Вас есть личные макеты, которые нужно дополнить реальностью, пришлите их нам и мы сможем понять, подойдут ли они. Если их нет, мы сами готовы их воплотить, учитывая все Ваши пожелания. Оформление личного сайта с помощью виртуальной и дополненной реальности не только поражает покупателя, но и даёт понять показатель подхода к управлению бизнеса. Тем самым Вы сможете отличиться среди других на рынке и четко заявить о себе.
is remeron a narcotic
Мобильное приложение дополненной реальности w2w.group
По запросу применения технологии дополненной реальности Вы на правильном пути. Наши консультанты готовы дать обратную связь и ответить на все оставшиеся вопросы. Если у Вас есть собственные образцы, которые нужно дополнить реальностью, пришлите их нам и мы сумеем понять, годятся ли они. Если их не существует, мы самостоятельно готовы их воплотить, учитывая все Ваши планы. Оформление личного сайта с помощью виртуальной и дополненной реальности не только удерживает покупателя, но и даёт понять уровень подхода к ведению бизнеса. Тем самым Вы сможете отличиться среди конкурентов на рынке и публично заявить о себе.
what is robaxin used to treat
sandyterrace.com
모든 것이 단순하게 유지되었기 때문에 그들을 환영하는 사람들이 너무 많지 않았습니다.
Холодильник Stinol – это не просто бытовой прибор, а незаменимый помощник на кухне, который позволяет сохранять свежесть продуктов питания. Если ваш холодильник начал барахлить, доверьте его ремонт профессионалам из stinol-servise.ru. Мы быстро и качественно устраним любую неисправность, восстановив нормальную работу вашего холодильника и продлив его срок службы.
ремонт холодильников stinol
замена термостата в холодильнике стинол цена
замена термостата в холодильнике цена стинол
buy metformin online canada
Создание визуальных впечатлений для Вашего бренда w2w.group
По поводу разработка приложений дополненной реальности мы Вам непременно окажем помощь. Вот уже свыше 6ти лет мы реализуем работу в данной сфере, имеем много позитивных комментариев и радостных покупателей, также успели воплотить более 120ти отличных проектов и всё с помощью новейших современных технологий. Ознакомиться с портфолио можно также на вышеупомянутом веб портале.
tadalafil 20mg buy
Использование виртуальной реальности w2w.group
По вопросу дополненная реальность в обучении Вы на верном пути. Наши консультанты готовы дать обратную связь и ответить на любые вопросы. Если у Вас есть личные макеты, которые нужно дополнить реальностью, пришлите их нам и мы сможем понять, подойдут ли они. Если их не существует, мы сами можем их создать, учитывая все Ваши планы. Оформление личного сайта с помощью виртуальной и дополненной реальности не только удивляет клиента, но и даёт оценить уровень подхода к управлению бизнеса. Тем самым Вы сможете выделиться среди конкурентов на рынке и громко заявить о себе.
protonix vs pepcid
synthroid price in india
What is FlowForce Max? FlowForce Max Advanced Formula is a holistic blend designed to promote optimal prostate health
I likewise think thus, perfectly written post! .
Good – I should certainly pronounce, impressed with your site. I had no trouble navigating through all tabs and related info ended up being truly simple to do to access. I recently found what I hoped for before you know it at all. Reasonably unusual. Is likely to appreciate it for those who add forums or anything, website theme . a tones way for your client to communicate. Nice task..
azithromycin 500mg tablets for sale
repaglinide medline india
ilogidis.com
Liu Jie는 여전히 불안감을 느끼며 시험실에 들어갔다.
lisinopril 40 mg mexico
bmipas.com
このブログは常に私に新しい知識をもたらしてくれます。感謝しています。
24 часа в сутки вывозим мусор ecologia-t.ru
По теме вывоз строительного мусора 8 м3 цена Вы на нужном пути. Осуществляем вывоз мусора разного вида: строительный, твердые бытовые отходы, металлолом, порубочные остатки, снег и другие. Также проводим работу 24 часа в сутки, без выходных и даже в праздничные дни. Делаем как разовые вывозы, так и ежедневные по определенным дням или часам, в зависимости от целей заказчика. Подходим к каждой проблеме персонально, чтобы реализовывать работу очень качественно.
qiyezp.com
공원에서는 모든 이름이 드러나기 시작했고 순위가 정해졌습니다.
Мусор Москва ecologia-t.ru
Относительно вывоз мусора контейнер 8 м3 москва мы Вам окажем помощь в данный момент. Звоните по контактному номеру телефона 8(495)506-26-76 или оформите обратный и мы Вам сразу перезвоним. Мы находимся по адресу: 109382, г. Москва, ул. Краснодонская, д. 46. Полный прайс лист Вы сможете найти на данном сайте ecologia-t.ru и зависит от многих показателей. Конкретно: тип мусора, размеры контейнера и требуемая грузоподъемность транспорта. Итоговая цена будет рассчитана после созвона с нашим специалистом. Звоните и прямо сейчас заполняйте заявку на вывоз мусора.
Заключить договор на вывоз мусора Москва ecologia-t.ru
Относительно аренда мусорного контейнера мы Вам окажем помощь в настоящий момент. Звоните по телефону 8(495)506-26-76 или закажите обратный и мы Вам перезвоним. Мы находимся по адресу: 109382, г. Москва, ул. Краснодонская, д. 46. Полный прайс лист Вы сможете найти на нашем сайте ecologia-t.ru и зависит от нескольких факторов. Это: вид мусора, объем контейнера и запрашиваемая грузоподъемность авто. Итоговая цена будет высчитана после общения с нашим менеджером. Звоните и скорее заполняйте заявку на вывоз мусора.
Вывезем любой мусор Москва ecologia-t.ru
По запросу вывоз промышленного мусора Вы на правильном пути. Вывозим отходы любого вида: смешанные отходы, твердые коммунальные отходы, стекольный бой, грунт, снег и другие. Также работаем круглосуточно, без выходных и даже в праздничные дни. Выполняем как одноразовые вывозы, так и постоянные по определенным дням или часам, в зависимости от целей клиента. Подходим к каждой проблеме индивидуально, чтобы выполнять работу максимально ответственно.
Недавно обращался в сервисный центр Zanussi по адресу zanussi-rem.ru. Мастера быстро диагностировали проблему и устранили ее всего за пару дней. Цена ремонта оказалась весьма приемлемой , а качество работы – на высоте . Теперь моя стиральная машина работает как новая . Искренне благодарю специалистов из сервиса Zanussi за профессионализм и оперативность!
175 mg synthroid
online prednisone
synthroid 0.15
prednisone brand
prednisone
synthroid 88 mcg cost
[url=http://ametformin.com/]buy metformin online mexico[/url]
synthroid 50 mcg price
metformin cheapest price
buy prednisone online canada
synthroid 0.0125 mg
synthroid 0.05 mg tablets
synthroid buy online uk
prednisone generic cost
zithromax online
lisinopril 20mg pill
where can you buy synthroid
buy metformin 500 mg online
synthroid 1mg
iv prednisone
lisinopril 40 mg mexico
prednisone purchase online
buy prednisone 5mg canada
compare synthroid prices
synthroid 100 mg cost
azithromycin otc in us
azithromycin purchase online
prednisone 54
synthroid 132 mg
buy metformin from mexico
prednisone 50 mg tablet
synthroid purchase online
lisinopril 40 mg daily
zestril brand name
zithromax 250 capsules
price synthroid 50 mcg
zestril brand name
lisinopril brand name
0.137 mg synthroid
best generic tadalafil
lisinopril 20 mg price in india
otc synthroid
lisinopril 10 mg daily
how to get glucophage
synthroid price uk
prednisone 50mg cost
price of prednisone
generic tadalafil australia
1.5 prednisone
cheapest synthroid prices
synthroid cost in canada
prednisone coupon
tadalafil 10mg daily
tadalafil 100mg online
azithromycin cost australia
purchase azithromycin 500 mg
generic zestril
buy lisinopril
lisinopril 5 mg coupon
top mail order pharmacies
online synthroid
buy prednisone india
best price for tadalafil
metformin how to buy
synthroid 0.025 mcg
where to buy prednisone
can you buy metformin in mexico
zestoretic 10 12.5 mg
prednisone over the counter
tadalafil
tadalafil brand
zestril pill
synthroid 60 mg
where can i get prednisone
canada metformin
where can i buy prednisone over the counter uk
where can i order lisinopril online
buy zithromax 250mg
prednisone 50 mg tablet
synthroid 100 mcg coupon
azithromycin buy online
online prednisone 5mg
lisinopril 20 tablet
cost of zithromax 500 mg
synthroid 200 mcg tablet
azithromycin 500mg buy
online order prednisone 10mg
tadalafil india 5mg
buy prednisone online australia
where to buy metformin online
20 mg prednisone tablet
synthroid 0.025 mg
synthroid 50mcg coupon
synthroid online coupon
azithromycin cost australia
prednisone 40
azithromycin generic cost
metformin over the counter uk
tadalafil 5mg uk
lisinopril generic over the counter
lisinopril 40 mg price
synthroid 0.025 mg
prednisone 200 mg daily
price of lisinopril
azithromycin 500 mg coupon
buy zestoretic
prednisone 10 mg
medication lisinopril 20 mg
metformin 50
synthroid 188
tadalafil generic canada
synthroid 112 mcg canada
can you buy azithromycin over the counter nz
50 mg prednisone tablet
synthroid generic brand
tadalafil for sale online
1 lisinopril
prednisone purchase
buy azithromycin tablet 500mg uk
lisinopril cheap price
azithromycin otc uk
azithromycin 250mg tabs
drug synthroid
otraresacamas.com
このような高品質な記事を提供してくれてありがとうございます。
metformin buy online australia
tadalafil gel
2 synthroid
medication lisinopril 10 mg
synthroid 201
synthroid 0.088 mg
buy metformin online india
tadalafil generic south africa
sandyterrace.com
곧 Ma Wensheng은 많은 엄격한 시선을 맞이했습니다.
lisinopril 20mg tablets
buy tadalafil 5mg
100 mg prednisone daily
where to buy metformin in usa
tadalafil australia paypal
zithromax 500mg online
generic zestril
order prednisone 10 mg tablet
cost for 2 mg lisinopril
Когда моя кофемашина Bosch сломалась, я сразу обратился в официальный сервисный центр Bosch. Там мне предложили бесплатную диагностику и быстрый ремонт. Очень порадовал профессионализм персонала и оперативность обслуживания. Кофемашина была отремонтирована в кратчайшие сроки, и мне еще и продлили гарантию на новые компоненты. Я остался полностью удовлетворен работой сервиса и качеством обслуживания.
Бош-Ремонт.рф – ремонт техники bosch
buying metformin online
lisinopril online canada
metformin 227
metformin 1000 mg price in canada
buy zestril online
can i purchase azithromycin over the counter
prednisone 10mg online
cheap meds metformin
tadalafil prices canada
lisinopril 420 1g
metformin purchase canada
lisinopril generic brand
buy cheap prednisone
where to get zithromax over the counter
how much is zithromax 250 mg
lisinopril brand name uk
generic tadalafil medication
synthroid drug
tadalafil
zestoretic 20 price
metformin 5 mg
happy family drug store
Когда моя стиральная машина Bosch начала издавать странные звуки во время стирки, я сразу же вызвал мастера из официального сервисного центра. Оказалось, что нужна замена подшипников. Ремонт прошел гладко, и машина теперь работает безупречно. Мастер был очень внимательным и профессиональным, все объяснил и показал. Доволен, что обратился именно к ним, работа сделана на совесть.
Бош-Ремонт.рф – ремонт кофемашин bosch
tadalafil 5mg uk
prednisone 10 mg tablets
lisinopril pill 40 mg
azithromycin 500 mg tablet buy online
cortisol prednisone
order lisinopril online us
synthroid 50 mcg tablet
where can i get azithromycin over the counter
buy lisinopril 10 mg online
cost of lisinopril 10 mg
tadalafil 20 mg tablet price
zestoretic 10 12.5 mg
synthroid 100 mg prices
lisinopril 5 mg for sale
azithromycin buy online india
buy azithromycin 1g
synthroid brand name price
synthroid 300 mcg tablets
brand name drug prednisone
synthroid 88 mcg
glucophage 850 online
synthroid buy
zithromax order online uk
buy azithromycin online
cheapest price for lisinopril
prednisone 50 mg tablet cost
tadalafil 5mg daily
best online tadalafil
metformin tab price
zithromax capsules buy
prednisone acetate
synthroid lowest price
tadalafil tab 10mg
synthroid 125 mcg
prednisone 5mg tablets
can you purchase azithromycin online
prednisone 20 tablet
is remeron an antipsychotic
order metformin usa
azithromycin without rx
synthroid 125 mcg price
prednisone daily
buy generic tadalafil online
metformin 1000 tab
azithromycin cost canada
azithromycin buy online
lisinopril cost uk
how can i get azithromycin
10mg generic 10mg lisinopril
azithromycin price australia
prednisone drugs
buying tadalafil in mexico
prednisone purchase online
how much is synthroid
200 mg prednisone daily
prednisone 20 mg in india
synthroid 75 mg price
synthroid 50 mcg tablet
can you buy azithromycin over the counter
zithromax generic cost
azithromycin coupon
lisinopril 5 mg daily
tadalafil soft 40 mg
buy zithromax over the counter
prednisone 20 mg
synthroid 10 mcg
cheap generic tadalafil 5mg
prednisone 20mg cheap
fake synthroid
online tadalafil
can you buy synthroid over the counter
synthroid 0.112 mcg
azithromycin 500 mg coupon
cheap prednisone online
prednisone brand name in india
lisinopril 20 mg tablets
canada buy prednisone online
prednisone 5mg price
where can i get azithromycin tablets
cheap glucophage
metformin online purchase
tadalafil cost in india
spironolactone side effects women
lisinopril 120mg
lisinopril tabs 20mg
tadalafil 20 mg no rx
otc synthroid
zestril over the counter
levothyroxine 50 mcg
price of zithromax
lisinopril tab 100mg
zithromax 500mg for sale
zithromax 250 mg price
generic prednisone cost
prednisone 20 mg pill
lisinopril 40 mg generic
where can i buy prednisone over the counter
lisinopril 20 mg best price
cost of lisinopril 5 mg
synthroid tablets 25 mcg
Мне хотелось бы от всего сердца поблагодарить ремонт ноутбуков в балашихе за их профессиональный подход. Они быстро и качественно отремонтировали мой ноутбук, и теперь он работает как новенький. Сотрудники были вежливыми и внимательными, подробно разъяснив мне все нюансы проведенного ремонта. Результат превзошел все мои ожидания, и с радостью порекомендую этот сервисный центр своим друзьям и знакомым
prednisone buy online
where can i get metformin in south africa
zestril cost price
synthroid discount
Столкнулся с проблемой в холодильнике Gaggenau: перестал морозить верхний отсек. Сервисный центр Gaggenau предложил оперативный выезд мастера. Специалист быстро нашёл неисправность — проблема была в системе No Frost, которую заменили на месте. Ремонт прошёл быстро, с гарантией на выполненные работы на год. Отличный сервис и профессиональный подход!
Gaggenau-Remonty.ru – сервисный центр gaggenau
buy prednisone with paypal
online prednisone
cost of prednisone in canada
metformin 1000 pill
cost for generic lisinopril
cheapest lisinopril 10 mg
synthroid 0.75 mg
prednixone tables for sale
generic synthroid canada
prednisone drug
prednisone corticosteroids
can i buy zithromax over the counter in canada
zithromax australia
price of metformin
synthroid cheap price
lisinopril 20mg tablets price
azithromycin 250 price
lisinopril price
best price for synthroid 50 mcg
tadalafil tablets in india online
synthroid 0.75
synthroid generic brand
prednisone 20mg cheap
generic tadalafil 10mg
azithromycin over the counter price
[url=http://isynthroid.online/]synthroid 88 mg[/url]
where to buy tadalafil in india
can i buy prednisone online
tadalafil 100mg best price
synthroid nz
При возникновении неисправностей с духовкой Gaggenau, вы можете рассчитывать на качественный ремонт с гарантией. В Москве многие сервисные центры предлагают послегарантийный ремонт этой техники. Специалисты не только быстро и точно диагностируют проблему, но и выполняют ремонт, используя исключительно оригинальные запчасти от производителя. Это обеспечивает не только долговечность ремонта, но и предоставляет гарантию на вновь установленные детали и выполненные работы.
Gaggenau-Remonty.ru – гагенау официальный сайт ремонт
buy metformin over the counter
synthroid cost generic
order synthroid
synthroid 88 mg price
buy synthroid 150 mcg online
synthroid 75 mcg tablet
synthroid 88 mcg cost
Моя посудомоечная машина Bosch начала шуметь и плохо сливать воду. Оказалось, что проблема в насосе. После недолгих поисков в интернете нашёл сервис, где мне предложили замену насоса по вполне приемлемой цене. Мастер приехал на следующий день, быстро и качественно провёл все работы. Цена оказалась точно такой, как и обговаривали изначально, без неприятных сюрпризов.
Бош-Ремонт.рф – сервис бош
where to buy metformin in usa
synthroid discount
Моя стиральная машина Bosch начала издавать необычный шум во время работы. Обратившись в надежный сервис, я получил выгодное предложение по ремонту с использованием оригинальных запчастей. Мастера приехали в удобное для меня время, провели качественный ремонт по доступной цене, благодаря чему машина была восстановлена до идеального состояния. Эффективность и экономичность услуги сделали этот опыт исключительно положительным.
Бош-Ремонт.рф – сервисный центр бош
buy azithromycin us
tadalafil 2.5
prednisone for dogs
synthroid cheapest prices
best prices for synthroid
how much is prednisone 20 mg
lisinopril tabs
brand synthroid
lisinopril 10 12.55mg
can i buy lisinopril online
order prednisone 10 mg tablet
prednisone 5
cost of generic lisinopril
prednisone tablets 5mg price
lisinopril 20 mg prices
prednisone 10mg tablets
average cost of metformin
prednisone tablets canada
lisinopril 102
synthroid drug
synthroid cost in canada
azithromycin where can i buy
lisinopril cheap brand
prednisone price australia
azithromycin buy us
synthroid online canada
lisinopril drug
how can i get zithromax
synthroid 0.137
4mg prednisone daily
prinivil 10 mg tablet
tadalafil 20mg best price
how to get prednisone online
buy synthroid australia
apo-prednisone
synthroid brand name cost
zestril 5 mg prices
lisinopril 20mg
prednisone 20 mg over the counter
Нужен срочный и недорогой ремонт холодильника Gaggenau в Москве? Сервисные центры предлагают оперативные и качественные услуги по доступным ценам. Мастера готовы приехать на дом в кратчайшие сроки, чтобы диагностировать и устранить любые неполадки. Благодаря использованию профессионального оборудования и оригинальных запчастей, ремонт выполняется быстро и эффективно, что позволяет восстановить работоспособность техники без значительных затрат. В результате вы получаете полностью функционирующий холодильник, готовый к дальнейшей эксплуатации.
Gaggenau-Remonty.ru – ремонт кофемашин gaggenau
30mg lisinopril
Если вы ищете профессиональный сервис по обслуживанию холодильников известной марки в столице, то вы пришли по адресу. Наш мастерская специализируется на восстановлении холодильного оборудования данной марки и имеет большой опыт в данной области. Мы гарантируем высокое качество услуг, применение фирменных запасных частей и умеренные тарифы. Обратитесь с нами прямо сейчас, и мы поможем вашему холодильнику Whirlpool функционировать как новенький! Для получения дополнительной информации посетите ремонт холодильников whirlpool.
order lisinopril online from canada
Выбирая сервисный центр Gaggenau для ремонта своей техники, я оценил их предложение о гарантии на 1 год. Это дало мне уверенность в долгосрочной работоспособности отремонтированных устройств. Специалисты быстро устранили неисправность моего паровара, и я получил официальную гарантию на выполненные работы. Такой подход подтверждает их ответственное отношение к качеству и клиентам.
Gaggenau-Remonty.ru – ремонт холодильников гаггенау
brand name azithromycin
can i buy synthroid over the counter
cost of tadalafil 5mg
order metformin on line
buy zithromax 1000 mg online
generic tadalafil in usa
cost of synthroid 75 mcg
100 mg lisinopril
cheapest synthroid prices
prednisone 40
buy synthroid 150 mcg
cougarsbkjersey.com
日常生活で直接役立つ実用的な情報が豊富で、素晴らしい記事です。
synthroid 125 mcg price
sitagliptin 50/1000
prinivil 20mg tabs
metformin online usa
synthroid 0.125 mg tablet
tadalafil 10mg price
where can you get azithromycin over the counter
cost of generic lisinopril
azithromycin 25 mg tablet
metformin over the counter south africa
buy tadalafil 20
where can i buy prednisone
generic synthroid prices
zestoretic 10 12.5 mg
prednisone 25mg from canada
zestril online
prednisone nz
synthroid india
glucophage costs
synthroid 0.0125 online
lisinopril price
synthroid cheapest prices
synthroid rx coupon
lisinopril 10 12.5 mg
6 metformin
discount zestril
where to buy synthroid online
cost of prednisone in canada
lisinopril 20mg for sale
drug lisinopril
azithromycin purchase canada
1000 mg zithromax online
buy lisinopril 10 mg uk
tadalafil rx
metformin 590 mg
how much is zithromax 500mg
can i buy prednisone over the counter in mexico
buy lisinopril 2.5 mg online
metformin 1500 mg
can i buy azithromycin in mexico
synthroid 125 mg cost
prices of metformin
prinivil drug
buy tadalafil tablets 20 mg
buy synthroid 150 mcg
lisinopril buy in canada
lightheaded synthroid
lisinopril tablet
buy synthroid online cheap
prednisone 20 mg
synthroid 137 mcg tab
metformin 143
zestoretic drug
buy prednisone online australia
buy generic tadalafil online cheap
brand name drug prednisone
lisinopril 10 mg tablet cost
buy prednisone tablets uk
how can i get zithromax over the counter
synthroid 50 mcg cost
generic azithromycin
tadalafil 20 mg tablet cost
glucophage
generic azithromycin
order azithromycin online usa
azithromycin 500 mg tablets
average price of prednisone
tadalafil price 5mg
prednisone 200 mg tablets
zithromax price in india
synthroid tablet 125 mcg cost
buy lisinopril 40 mg tablet
azithromycin paypal
mikaspa.com
Hongzhi 황제는 도울 수 없었지만 그를 쳐다 보았고 그의 눈썹은 더욱 깊어졌습니다.
lisinopril 40 mg price
prednisone mexico
synthroid in india
buy zestril 20 mg online
tadalafil tablets in india online
tadalafil mexico
order lisinopril
synthroid 50 mcg coupon
azithromycin 500g tablets
synthroid brand name cost
synthroid tabs 88 mcg
synthroid 88 price
prinivil 10 mg
best price for synthroid 100 mcg
lisinopril brand
buy prednisone
azithromycin capsules
can i buy azithromycin over the counter in us
synthroid discount coupon
tamsulosin erectile
amoxicillin azithromycin
lisinopril 20 mg india
where can i buy zithromax online
synthroid 0.175 mg
order cheap lisinopril
synthroid 75 mcg tablet price
prednisone 16 mg
prednisone 30g
synthroid 62.5 mcg
tadalafil price uk
best price for lisinopril 20 mg
venlafaxine and wellbutrin
prednisone price canada
synthroid 75 mcg cost
purchase lisinopril 40 mg
zithromax tablets australia
glucophage generic
prednisone 1mg purchase
prednisone acetate
zestoretic 20 25 mg
best tadalafil brand in india
lisinopril 2.5 mg coupon
azithromycin tablets over the counter
cheap metformin online
azithromycin 1000mg
cost of generic zithromax
zestril generic
buy prednisone 10mg tabs
synthroid 175 mcg tab
how much is zithromax 500mg
zithromax tablet 500mg
can i buy synthroid over the counter
discount zestril
synthroid 10 mcg
prednisone 25 mg tabs
cheap tadalafil 20mg
price for 15 prednisone
zestril 10 mg cost
azithromycin prices in india
qiyezp.com
Zhang Lai는 안도의 한숨을 쉬었습니다. 이것이 바로 그것입니다. 완벽하게 일치하는데 문제가 무엇입니까?
tadalafil canada drug
generic zestoretic
azithromycin buy india
generic metformin price
synthroid 1mg
buy synthroid online usa
prednisone rx
order lisinopril
predisone with no presciption
tadalafil india online
prednisone 4 tablets daily
cheap zithromax online
prednisone 1 mg price
tadalafil 5 mg tablet coupon
synthroid 0.125 mg
tadalafil 10mg daily
tadalafil 5mg canada
azithromycin price south africa
best price for synthroid 137 mcg
lisinopril mexico
tadalafil tablets 20 mg
lisinopril 20 mg online
zithromax 500mg price in india
tadalafil uk generic
tadalafil 60 mg
buy metformin without a proscription
500 mg azithromycin
tadalafil 20mg canadian
can i buy prednisone over the counter in mexico
buy azithromycin tablets in us
buy azithromycin 250 mg
how much is lisinopril 20 mg
buy synthroid online from canada
azithromycin for sale online
will tizanidine show up on a drug test
prednisone 100 mg tablet
buy metformin
lisinopril cost 40 mg
synthroid for sale
lisinopril 10 mg brand name in india
synthroid 62 5 mcg
zestoretic 20 12.5 mg
tadalafil us
lisinopril online canada
prednisone in india
metformin online usa
prednisone cost
lisinopril brand
prinivil 10 mg
buy prednisone nz
azithromycin z-pak
buy tadalafil 40 mg
reputable overseas online pharmacies
prednisone 2 mg
prednisone 477
Изучите список всех новых займов, которые можно получить на карту без проверки кредитной истории и без риска отказа. Эти предложения от новых МФО идеально подходят для тех, кто сталкивается с временными финансовыми трудностями и нуждается в быстром решении. Благодаря упрощенным условиям и отсутствию строгих проверок, каждый может получить необходимую сумму с минимальными затратами времени.
Фин-Мир малоизвестные мфо предоставляющие займы онлайн
cost of synthroid in canada
lisinopril 50 mg tablet
can i buy azithromycin over the counter in us
metformin 227
synthroid 05 mg
is thera a generic for voltaren gel?
where can i buy metformin online uk
prednisone buy cheap
buying online metformin from india
azithromycin online
synthroid 125 coupon
can you buy prednisone over the counter in canada
how to get zithromax online
price of prednisone
prednisone 5mg price
prednisone tabs
5mg tadalafil from canada
synthroid 0.125 mcg
prednisone 5052
discount zestril
order azithromycin from mexico
20 mg lisinopril tablets
compare synthroid prices
synthroid 88 mcg cost
prednisone 20 mg tablet price
lisinopril 10 mg canada cost
lisinopril 20 mg tablet cost
synthroid for sale usa
metformin 142
synthroid tablet 125 mcg cost
how to order metform onlline
lisinopril 40 mg for sale
can i buy synthroid online
tadalafil 20mg mexico
lisinopril 20 mg sale
buy synthroid 112 mcg
prednisone 50
metformin online australia
prinivil 5 mg
azithromycin otc
fpparisshop.com
この記事の書き方が大好きです。明確で分かりやすい。
zestoretic 10 mg
prednisone from india
zithromax 600 mg
synthroid 0.05mg tablet
cost of synthroid generic
azithromycin 500mg tablets for sale
synthroid 75 mg coupon
prinivil 20 mg
canadian price for synthroid
drug metformin
price of lisinopril 20 mg
prednisone pill
prednisone medication
cheap synthroid
5mg prednisone
synthroid 137.5 mcg
tadalafil 30
zithromax otc
buy zithromax online usa
mikaspa.com
정신과를 제외한 나머지 과들은 사람들로 붐볐다.
prednisone 50 mg buy
lisinopril 2.5 mg price
synthroid 62.5 mcg
how can i get metformin
generic tadalafil south africa
glucophage medication
average cost of lisinopril
depakote and zyprexa together
lisinopril 60 mg
tadalafil india paypal
azithromycin order online
synthroid 100 mcg online
prednisone 40 mg rx
prednisone 30 mg coupon
buy generic lisinopril
tadalafil 30mg tablet
tadalafil 5mg in india
cheap synthroid
wellbutrin interactions with caffeine
prednisone australia
buy prednisone online uk
prinivil 10 mg
zestril price
50 mg lisinopril
where to buy zithromax online
cost of synthroid 200 mcg
142 metformin
lisinopril 49 mg
azithromycin capsules 500mg
tadalafil 20 mg soft tabs
synthroid 25
how much is tadalafil
metformin buy
cheap metformin online
azithromycin from mexico
synthroid lowest price
cost of lisinopril 30 mg
synthroid 1.25 mcg
tadalafil 100mg price
synthroid 1
synthroid prices
cost of synthroid 175 mcg
synthroid 125 mcg coupon
metformin price
how can i get zithromax over the counter
prednisone 2.5 mg tab
can you buy tadalafil online
synthroid cheap price
zithromax 250 mg cost
generic tadalafil 20mg for sale
cost synthroid
synthroid 125 mg coupon
lisinopril 1.25
synthroid 100 mcg price in india
synthroid purchase online
synthroid 1 mg
lisinopril 40 mg brand name
order prednisone online
tadalafil buy online canada
can i buy lisinopril online
metformin 850 mg price in india
prednisone 2.5mg tab
synthroid 30 mg
synthroid 150 mcg
prednisone brand name australia
cost of prednisone in canada
azithromycin 250mg tablets cost
zithromax order
tadalafil online price
buy azithromycin from mexico
lisinopril 10 best price
can i buy synthroid online
generic zofran images
buy metformin 500 mg
top 10 pharmacies in india
buy azithromycin online australia
metformin sr
zestoretic online
metformin 50 mg tab
lisinopril 49 mg
lisinopril 5 mg for sale
lisinopril hctz
cost of azithromycin
lisinopril 30
lisinopril 10 mg canada cost
lisinopril generic drug
tadalafil brand name
prednisone brand name cost
lisinopril 3972
metformin otc mexico
where can i buy zestril
can you buy prednisone over the counter in mexico
cost of tadalafil 20 mg
tadalafil prices 5mg
synthroid best prices
synthroid 88 mcg
synthroid 250 mg
synthroid 88 mcg tab
buy prednisone with paypal
cost of generic synthroid
cost of tadalafil 20 mg
azithromycin paypal
how can i get zithromax
zithromax no rx
lisinopril 20 mg for sale
lisinopril 28 mg
over the counter synthroid
cheapest tadalafil online compare prices
where can you buy prednisone
azithromycin drug
lisinopril without an rx
metformin tablets in india
order prednisone from canada
order tadalafil tablets 20 mg
synthroid 110 mcg
prednisone uk
synthroid lowest prices
purchase metformin online
tadalafil buy online canada
synthroid 50 mcg in india
tadalafil 600 mg
best online tadalafil
azithromycin 500mg tablets online
synthroid medication
buy zithromax online fast shipping
lisinopril 30
tadalafil brand
lisinopril 5 mg tablet
prednisone 5mg price
prednisone brand
lisinopril 5mg cost
synthroid lowest prices
metformin 850 mg buy online
glucophage tab 850 mg
tadalafil generic india
lisinopril 10mg
120 mg prednisone
can you buy metformin over the counter
zestril 10
zithromax z pack
cost of synthroid generic
synthroid 150 mcg cost
137 mg synthroid
tadalafil 60 mg
average cost of glucophage
lisinopril cost uk
zestril 40 mg tablet
cost of synthroid medication
prednisone for sale 5mg
where to buy synthroid
generic tadalafil uk
buy prednisone online
cheapest price for lisinopril
metformin 5000 mg
25 mg prednisone
generic tadalafil from canada
generic tadalafil safe
buying prednisone
buy lisinopril 10 mg
prednisone buy cheap
what is zetia
best price for synthroid 50 mcg
120 prednisone
prednisone 25
lowest price for synthroid 88 mcg tablet
prednisone 10mg pack
buy tadalafil paypal
lisinopril medication
synthroid 60 mcg
synthroid 25 mg
generic drug for lisinopril
tadalafil 10 mg tablet
lisinopril tablets
buy metformin 850 mg online
lisinopril 40 mg daily
lisinopril 5 mg tablet price in india
zithromax 250mg online
tadalafil online without a script
metformin 143
lisinopril
metformin canada online
cost of prednisone tablets
prednisone price in india
zestril 2.5
I gotta favorite this web site it seems invaluable very beneficial
prednisone 5084
40 mg prednisone daily
can i buy prednisone online
synthroid 88 mcg price
cost of lisinopril 20 mg
lisinopril 1.25 mg
lisinopril 30 mg cost
metformin hcl 1000mg
tadalafil 20mg price
price of synthroid
fpparisshop.com
素晴らしい記事!とてもインスピレーションを受けました。
over the counter tadalafil usa
azithromycin 500mg tab price
buy azithromycin in usa
lisinopril 5mg buy
metformin script
metformin 104 pill
synthroid 30 mg
azithromycin 500 prices
prednisone10 mg
buy azithromycin 1000 mg
prednisone cost canada
lisinopril hct
synthroid 137 mg
average price of prednisone
prednisone 300 mg
zestril tab 10mg
5mg prednisone
generic azithromycin over the counter
azithromycin over the counter in us
where can you buy azithromycin 500mg
zithromax uk online
prednisone pill cost
lisinopril 1.25 mg
where can i get azithromycin
lisinopril 20
can i take zofran and pepcid together
generic tadalafil 40 mg
azithromycin capsules 500mg
azithromycin brand name in canada
prednisone order online uk
synthroid 100 mcg tablet
buy tadalafil mexico online
azithromycin coupon
prednisone 20 mg brand name
prednisone 40 mg tablet
prednisone 10
synthroid 250 mg
buy tadalafil online
zestoretic 10 12.5 mg
buy tadalafil us
cost of azithromycin
[url=https://synthroidx.com/]levoxyl synthroid[/url]
iv prednisone
tadalafil 100mg
buy synthroid australia
metformin 500 mg brand name
synthroid price comparison
buying synthroid in mexico
can you buy prednisone over the counter
azithromycin purchase canada
how much is metformin 1000 mg
tadalafil 2.5 mg tablets in india
15 mg prednisone daily
zithromax over the counter canada
where can i buy metformin in south africa
prednisone where to buy uk
synthroid 75 pill
zithromax 750 mg
synthroid 100 mcg coupon
tadalafil india buy
buy cheap generic zithromax
where can i buy prednisone
how to buy tadalafil
prednisone price
on line order lisinopril 20mg
zestril 40 mg
buy lisinopril 20 mg online uk
prednisone 200 mg
lisinopril india
generic zithromax online paypal
how much is prednisone 5mg
prednisone 2.5 mg tablet
can you buy azithromycin over the counter in usa
can you buy azithromycin over the counter nz
buy tadalafil in australia
20 mg prednisone
how to buy prednisone
zithromax from mexico
can i buy lisinopril over the counter
zestoretic online
metformin 500 mg brand name
synthroid purchase
synthroid 200 mcg coupon
buy lisinopril online canada
tadalafil generic best price
synthroid 112 mg
synthroid 0.0125 online
where can you get azithromycin over the counter
cost for 40 mg lisinopril
synthroid cost
generic zestoretic
buy synthroid 75 mcg
tadalafil 10mg india
order lisinopril 10 mg
azithromycin 250mg generic cost
buy metformin 500 mg without a rx
prednisone generic brand name
tadalafil tablet buy online
glucophage 850
synthroid 0.075 mcg
cost of metformin 500 mg in india
tadalafil 50mg
tadalafil india online
price of lisinopril generic
can you buy zithromax online
metformin 13
metformin online purchase
tadalafil tablets buy
how to get metformin online
game1kb.com
Zhen Guo Mansion을 지배하는 사람은 명나라 총리가되는 것과 같습니다.
tadalafil 2
tadalafil cost uk
brand name azithromycin
lisinopril 25 mg
order metformin 1000 mg
azithromycin 500 mg generic price
metformin 500 mg price in india
cost of generic lisinopril 10 mg
metformin 500 mg price australia
[url=http://azithromycinps.online/]azithromycin tablets for sale[/url]
glucophage cheap
metformin 800
cost for generic lisinopril
lisinopril 10 12.5 mg tablets
how to get metformin online
zithromax 250 mg tablet price
zestril 20
price of metformin 500mg tablets
buy lisinopril 5mg
lisinopril 10 mg best price
[url=https://azithromycinmds.com/]azithromycin 500mg cheap[/url]
best tadalafil brand
tadalafil 10 mg tablet
zithromax z-pak
synthroid tablets for sale
metformin where to get
lisinopril 60 mg
metformin 600 mg
price of azithromycin 500 mg in india
zithromax canada
azithromycin online
synthroid 200 mcg cost
lisinopril 20 mg coupon
synthroid tabs 75mcg
synthroid 1mg
buy azithromycin online
azithromycin 500mg for sale
buy tadalafil canada
generic tadalafil cheap
order azithromycin online usa
lisinopril 2.5 cost
lisinopril online usa
lisinopril 20
lisinopril 49 mg
glucophage xr
buy synthroid online uk
synthroid tablet 125 mcg cost
prednisone 10 mg over the counter
synthroid generic canada
zithromax price canada
prednisone 2.5 mg tab
best generic synthroid
can you buy zithromax over the counter in mexico
lisinopril india
lisinopril 40 mg pill
Для тех, кто нуждается в профессиональный сервис по обслуживанию устройств Lenovo, обратитесь к lenovoserviset.ru. Опытные мастера справятся с любые проблемы, связанные с ноутбуками, планшетами и другими устройствами Lenovo. Вы можете рассчитывать на безупречное исполнение работ по доступным ценам.
tadalafil 10mg price
zithromax drug
buying synthroid in mexico
cost of prednisone
purchase zithromax online
daily prednisone
lisinopril 20 mg uk
order azithromycin 500mg
buy lisinopril 20 mg online uk
synthroid 137 pill
synthroid 0.175 mg
metformin buy online india
54899 prednisone
prednisone 12 tablets price
synthroid 112.5
zestril 5mg
prednisone 80 mg daily
azithromycin 1000 for sale
synthroid 100
zithromax buy online
prednisone 105mg
synthroid generic cost 100 mcg
synthroid 5 mcg
levoxyl synthroid
prednisone over the counter
azithromycin over the counter uk
azithromycin 500mg tablets for sale
cost of generic lisinopril
100 mg lisinopril
synthroid 137 cost
zestril 10mg
4mg prednisone daily
synthroid 500 mcg
synthroid generic cost 100 mcg
azithromycin 1g buy online
generic zestoretic
metformin otc usa
synthroid tab 88mcg
order azithromycin online
can you buy metformin over the counter in australia
prednisone 20mg tablets
prinivil lisinopril
prednisone tablet cost
azithromycin 250mg cost
can i buy prednisone over the counter
lisinopril 2.5 pill
metformin 500 mg coupon
synthroid 0.075 mg
azithromycin 1000 mg price
where can i buy synthroid
zestril 5 mg tablet
prednisone 5mg cost
zithromax for sale
synthroid 100 mcg
prednisone 543
prednisone 60
azithromycin over the counter price
prednisone 5 mg tablet price
lisinopril canada
tadalafil from india 5mg
synthroid generic
zestoretic 20 12.5 mg
generic prednisone tablets
tadalafil 20mg cheap online
buy generic zithromax
buy lisinopril online canada
synthroid 25
cost of synthroid 200 mcg
60 lisinopril cost
synthroid 0.025
metformin 1000 mg pill
Когда возникли проблемы с моим Lenovo, я нашел отличный сервисный центр – lenovoruremont.ru. Меня впечатлил высоким уровнем обслуживания и профессионализмом мастеров. Специалисты оперативно выявили неисправность и предложили оптимальное решение. Ремонт был выполнен качественно и в срок. Я очень доволен результатом и могу смело рекомендовать этот сервисный центр для ремонта устройств Lenovo.
lisinopril 10mg tablets
buy prednisone without rx
lisinopril 10 mg canada
where to purchase tadalafil
where can i buy prednisone over the counter uk
lisinopril 5mg tabs
tadalafil soft
tadalafil 20 mg no rx
cost of synthroid mexico
lisinopril online uk
prednisone buy online
tadalafil buy online
azithromycin z pack
azithromycin 2g
buying metformin online
zithromax 250 mg pill
synthroid 25 mg tablet
purchase synthroid online
metformin india
tadalafil 7.5 mg
prednisone 10mg for sale
synthroid pill 88mg
prednisone corticosteroids
prednisone 60 mg cost
tadalafil 20 mg soft tabs
cost of generic zithromax
synthroid in india
cheap prednisone
tadalafil for sale online
price of tadalafil 20mg
tadalafil 40 mg uk
synthroid 10 mcg
Great work! This is the type of info that should be shared around the net. Shame on Google for not positioning this post higher! Come on over and visit my site . Thanks =)
prednisone 25g
synthroid 135 mcg
synthroid 175 price
brand name synthroid coupon
azithromycin 500 mg tablet
metformin 500 mg tablet online
cheap generic tadalafil
prednisone 20mg tablets
synthroid cheapest price
where can you buy prednisone
generic tadalafil united states
prednisone 20 mg tablets coupon
tadalafil 10 mg tablet
metformin in europe
tadalafil tablets 20 mg india
prednisone 60mg daily
tadalafil 20mg lowest price
synthroid brand name
tadalafil 5mg generic
tadalafil 40 mg cheap
20 mg tadalafil buy
sandyterrace.com
수많은 사람들이 환호하고 둘러보았고, 군중은 동요하고 빠르게 물러났습니다.
onair2tv.com
이 향기는 분명히 Concubine Fang의 몸에서 가져온 것입니다.
best price for tadalafil 20 mg
prednisone 1 tablet
buy synthroid 75 mcg
tadalafil 5 mg
lisinopril 10 mg tablet cost
generic lisinopril 40 mg
metformin 1000 mg price india
lowest price tadalafil
metformin tablets for sale
prednisone brand name us
cheap glucophage
buy tadalafil 20mg online
metformin 250
synthroid cheapest prices
synthroid 20 mcg
buy synthroid online usa
synthroid canada price
metformin glucophage
price of prednisone
cheap synthroid
lisinopril 5 mg tablet
lisinopril 1.25 mg
zestril brand name
synthroid 15 mg
lisinopril 5 mg price
metformin 1000 mg pill
best metformin brand
zestril 5 mg tablet
tadalafil 7.5 mg
tadalafil for sale
order prednisone online
synthroid 25 mg cost
synthroid 112 mcg
buy tadalafil online australia
synthroid 500 mcg
canadian 5mg tadalafil online
metformin coupon
purchase lisinopril online
where can i buy lisinopril
lisinopril tabs 10mg
canadian pharmaceuticals for usa sales
canada prednisone 50 mg
generic tadalafil safe
lisinopril oral
synthroid 75 mg
cheap online tadalafil
azithromycin 600 mg tablet rx
Your place is valueble for me. Thanks!…
prednisone 1 tablet
metformin coupon
how to get zithromax
metformin online canada drug
prednisone 10 mg coupon
buy synthroid online uk
100 mg lisinopril
brand name synthroid price
prednisone in india
1g metformin
lisinopril 2018
lisinopril brand name canada
synthroid 110 mcg
prednisone 1 mg for sale
azithromycin tabs 500mg
azithromycin 600 mg tab
synthroid buy
lisinopril 20 mg price
purchase prednisone
prednisone canada prices
synthroid price canada
glucophage brand cost
prednisone in mexico
prednisone 20 mg tablet
6 azithromycin without rx
prednisone 5mg price in india
glucophage 500mg price
synthroid 112 mcg tablet
where can i get azithromycin tablets
average cost of generic prednisone
lisinopril tablet
azithromycin 1000
generic for zestril
otc metformin
buy lisinopril canada
medication lisinopril 5 mg
order tadalafil 20mg
legitimate canadian online pharmacies
tadalafil 10 mg
lisinopril 20 mg daily
prednisone 5 tablet
prednisone 5mg cost
order azithromycin online usa
otraresacamas.com
この記事の実用性は驚くべきものがあり、大変役に立ちました。
metformin 50
tadalafil soft tabs 20mg
azithromycin in canada
where can i get azithromycin 500 mg
prednisone 1 tablet
synthroid 137 price
synthroid 150 mg coupon
azithromycin tabs 250 mg
lisinopril 419
zithromax 500mg australia
lisinopril 60 mg daily
prednisone brand name in india
azithromycin 500mg tablets price in india
azithromycin 25 mg
lisinopril 10mg tablets
tadalafil 20mg india price
metformin 3115 tablets
buy synthroid
synthroid 0.112 mg
prednisone 473
can you buy prednisone over the counter
tadalafil 5 mg tablet coupon
glucophage 1000 mg
synthroid tablets 25 mcg
azithromycin cost
lisinopril 3.125
price of lisinopril 30 mg
buy glucophage 500mg
generic zithromax online
prednisone 1 mg cost
tadalafil 40 mg
azithromycin 250 mg suppliers
zithromax generic usa
tadalafil otc usa
azithromycin 25 mg cost
2 prinivil
112 mg synthroid
20mg daily prednisone
prednisone 20 mg tablet price
1 mg prednisone cost
synthroid rx coupon
prednisone 473
tadalafil canada generic
synthroid 100 mcg from canada
5094 prednisone
synthroid tablets 25 mcg
lisinopril pill 10mg
cost of metformin 500 mg
lisinopril 12.5 mg 10 mg
synthroid 30 mg
synthroid 50
purchase tadalafil
prednisone 5 mg buy online
112 mg synthroid
[url=https://asynthroid.com/]synthroid 75 mcg cost[/url]
buy tadalafil 100mg
discount generic tadalafil
synthroid 0.112 mcg
order lisinopril 20mg
synthroid 35
synthroid 25 mcg daily
lisinopril drug
synthroid 25 mcg cost
can you buy prednisone
generic synthroid
amoxicillin azithromycin
prednisone 25mg from canada
synthroid 125 mcg tablet
prinivil 2.5 mg
zestril 20 mg
azithromycin paypal
synthroid tab 88mcg
tadalafil 5mg cost
synthroid 125 mcg cost
where can i get azithromycin over the counter
azithromycin generic cost
metformin 500mg with out presciption
where to buy prednisone in canada
zestril 5 mg india
how to get azithromycin over the counter
10 mg prednisone
zithromax 250 price
lisinopril 5 mg price in india
buy synthroid cheap
zestoretic medication
[url=https://bestmetformin.online/]metformin 7267[/url]
canada generic tadalafil
best prednisone
tadalafil 2.5
synthroid 0.05 mg
bestmanualpolesaw.com
그가 막 들어가려고 했기 때문에 누군가 그를 말렸습니다.
metformin 3000 mg
zithromax tablets online
metformin 13
can i buy prednisone online in uk
buy prednisone nz
prednisone best price
synthroid 0.1 mg
how much is prednisone 5mg
synthroid 88 lowest cost
mail order prednisone
tadalafil tablets in india online
discount generic tadalafil
order azithromycin from mexico
cost of azithromycin
tadalafil generic where to buy
prednisone 10 mg prices
azithromycin 1000mg tablets
synthroid 25 mg daily
24 mg prednisone
prednisone purchase online
synthroid 225 online
generic tadalafil 5mg cost
prednisone 20 mg purchase
azithromycin 787
zithromax capsules 250mg
synthroid brand name price
order prednisone 10mg
prednisone over the counter in mexico
buy synthroid
azithromycin 250 mg price in india
buy synthroid online uk
tadalafil united states
azithromycin cap 250 mg
can you buy lisinopril over the counter
metformin 102
medication lisinopril 20 mg
average cost of azithromycin
cheap generic prednisone
azithromycin australia cost
prednisone 10mg online
zestril 40 mg
azithromycin 500 buy online
metformin purchase canada
112 mg synthroid
synthroid medication online
tsh synthroid
where to buy glucophage online
tadalafil generic usa
synthroid 0.088
buy zithromax online uk
buy metformin 850 mg
canada prednisone 50 mg
canadian drug prices for metformin
zestril lisinopril
metformin script cost
zithromax best price
metformin 100 mg price
Very interesting subject , thanks for putting up.
azithromycin lowest price
zithromax buy
prednisone online purchase
azithromycin 250 mg purchase
buy prednisone 10mg tabs
tadalafil 20mg coupon
buy tadalafil 20
metformin 750
synthroid online paypal
prednisone online india
1000 mg zithromax online
synthroid 200 mcg
175 mg synthroid
25 mg lisinopril
azithromycin 500mg tab cost
metformin 500 mg tabs
lisinopril 25 mg price
tadalafil tablets uk
prinivil 10 mg
prednisone 300 mg
lisinopril 40 mg india
synthroid 0.2 mg
750 mg metformin
azithromycin cost
buy lisinopril online
safe online pharmacies in canada
cost of prednisone tablets
where to buy prednisone 20mg
can i order metformin online
Nice post. I learn something totally new and challenging on websites
prednisone order online uk
lisinopril 10 india
lisinopril 125 mg
prinivil medication
azithromycin buy online
azithromycin price uk
synthroid drug
online tadalafil us
generic tadalafil 20mg for sale
buy metformin er
prednisone coupon
prednisone 50 mg tablet canada
synthroid tablets uk
cost of generic lisinopril
metformin without presription
buy azithromycin india
synthroid 88 mg
lisinopril online uk
synthroid 1.5
synthroid brand 88 mcg
synthroid 15 mg
glucophage tab 1000mg
drug azithromycin 500 mg
tadalafil 500mg
synthroid online uk
metformin 100 mg tablets
lisinopril cost canada
tadalafil buy canada
synthroid 25
synthroid order
buy generic synthroid online
tadalafil 10mg from canada
tadalafil 5mg cost
toasterovensplus.com
このブログのファンになりました。いつも新鮮で興味深い内容をありがとうございます。
lisinopril 3.125
geinoutime.com
오늘 밤 폐하를 볼 수 없다는 것이 유감스럽기 때문에 인내심을 가지고 내일 아침까지 기다려야 궁에 들어갈 수 있습니다.하지만 분명히 Fang Jifan은 이 문제를 더 적절하게 처리할 다른 방법을 생각해야 합니다!
lisinopril online uk
medication lisinopril 10 mg
synthroid 175 mcg
buy predisone steriods
generic tadalafil from uk
prinivil 40 mg
prednisone 40 mg price
metformin hcl 1000 mg
lisinopril 5mg prices
buy lisinopril online uk
metformin 100 mg
zestril 2.5 mg tablets
lisinopril tab 20mg cost
synthroid over the counter online
40 mg prednisone pill
prednisone 60mg daily
tadalafil 20mg price in usa
prinivil lisinopril
where to buy metformin 850 mg
synthroid 200
[url=https://isynthroid.com/]synthroid price india[/url]
buy prednisone online australia
synthroid 100 mcg price
lisinopril diuretic
metformin without rx
prednisone 20 mg buy online
cost of lisinopril in mexico
tadalafil canadian prices
prednisone 10 mg tablet
lisinopril online uk
zestril price uk
synthroid 1
metformin 1000 mg
zestoretic 20 25mg
how to get azithromycin over the counter
prednisone 60 mg
synthroid 250
can i buy metformin over the counter
zestril 5mg
otc metformin
metformin buy australia
prednisone 50 tablet
synthroid 115 mcg
prednisone 80 mg tablet
azithromycin 500mg tab cost
largestcatbreed.com
그 결과 오스트리아에 군대를 파견하기 위한 오스만의 군사비가 늘어나기 시작했다.
lisinopril 7.5 mg
preddisone no
metformin 1250 mg
metformin tablet price in india
prednisone 40 mg rx
metformin 142
lisinopril from canada
lisinopril in mexico
prinivil medication
buy metformin 1000 no rx
buy lisinopril 10 mg uk
can i buy azithromycin over the counter uk
lisinopril 422
lisinopril 10 mg price
lisinopril 5 mg
synthroid 0.5
metformin hcl 500mg
where to get tadalafil
metformin 850
buy tadalafil 20mg price canada
rx lisinopril
azithromycin price in mexico
cost of prednisone 20mg
synthroid 80 mcg
zestoretic 10 12.5 mg
azithromycin z-pack
20 mg lisinopril tablets
cheap generic synthroid
40 mg lisinopril
cheapest price for lisinopril
azithromycin 500mg cheap
how much is synthroid
generic zithromax online
1250 mg prednisone
tadalafil 2.5 mg tablet
tadalafil 20 mg best price in india
lisinopril
zithromax tablets price
buy tadalafil uk
lisinopril hctz
prednisone 25mg from canada
purchase lisinopril 40 mg
prednisone 250 mg
tadalafil 90 tabs
tadalafil 20 mg no rx for sale
buy prednisone mexico
tadalafil generic over the counter
prednisone daily
synthroid 50mcg
azithromycin uk
how to buy lisinopril online
zithromax tablets online
how to get azithromycin 500 mg
synthroid 275 mcg
azithromycin 500 buy online
metformin hcl 1000mg
lisinopril without an rx
azithromycin 100 mg sale
rx lisinopril
purchase lisinopril
order tadalafil online
cost of metformin uk
lisinopril pill 10mg
synthroid 35
buying synthroid in mexico
20 mg prednisone tablet
prednisone 30 mg tablet
synthroid 0.25 mg tablet
synthroid 112 mcg canada
37.5 mcg synthroid
metformin 101
azithromycin 250 mg for sale
brand synthroid
tadalafil price in mexico
synthroid 75 mcg price
buy tadalafil cheap
tadalafil coupon discount
buying prednisone mexico
steroids prednisone for sale
synthroid 12.5 mcg order online
zithromax india
buy synthroid 112 mcg
lisinopril pill
buy azithromycin over the counter
lisinopril price in india
prednisone
synthroid 50 mcg tab
medication synthroid
metformin 2000 mg daily
synthroid 50 mg
best azithromycin tablet
lisinopril 40 mg canada
synthroid online canada
azithromycin cheap online
azithromycin 600 mg tablet
buy synthroid 112 mcg
prednisone brand name canada
synthroid 0.125 mcg
where can i buy lisinopril
order azithromycin 500mg
buy tadalafil us
025 mg synthroid
prednisone 20 mg online
5mg prednisone daily
compare prednisone prices
can i order lisinopril online
azithromycin price canada
lisinopril tabs
buy prednisone online without a script
prednisone prices
azithromycin 25mg price
synthroid 201
lisinopril sale
azithromycin buy online us
azithromycin for sale canada
zithromax 1g
prednisone by mail
synthroid pill
india tadalafil comparison
best price zithromax 250mg
azithromycin 500mg price south africa
lisinopril 10 mg cost
50mg prednisone tablets
glucophage 850mg prices
how much is prednisone 20 mg
buy cheap generic zithromax
prednisone 60 mg
prednisone over the counter canada
order prednisone online
can you buy synthroid in mexico
tadalafil soft gel capsule
metformin 500 mg for sale
synthroid canada
tadalafil 30mg pill
prednisone generic brand name
tadalafil 10 mg coupon
zithromax canada
where can you buy synthroid
[url=http://tadalafilstd.online/]generic tadalafil coupon[/url]
buy metformin 1000mg
lisinopril 10 mg tablet
tadalafil 10mg india
cost of azithromycin in india
synthroid 150 mcg tab
tadalafil 5mg cost
synthroid pill
synthroid 50 mg cost
synthroid 88 mcg cost
tadalafil discount
synthroid 25 mcg daily
azithromycin generic cost
buy azithromycin tablet 500mg uk
how to get azithromycin online
buy cheap lisinopril 40 mg
prednisone buy canada
can i buy zithromax online
buy zithromax 500mg online
metformin 500 mg tablet
lipinpril
lacolinaecuador.com
그들이 늑대와 호랑이처럼 게걸스럽게 먹는 것을 지켜보십시오.
how to get synthroid
buy lisinopril 20 mg online united states
synthroid 175 price
synthroid 50
lisinopril 10mg
lisinopril in india
metformin price in india
buy lisinopril 5mg
glucophage 500mg price in india
can you buy prednisone over the counter in mexico
synthroid cost canada
lisinopril 20mg tablets
azithromycin 500 mg tablet brand name
cost of zithromax 500 mg
glucophage generic
tadalafil citrate
generic synthroid
synthroid 15 mg
can i buy synthroid over the counter
buy azithromycin usa
can i buy metformin over the counter in canada
zithromax india
tadalafil 20mg price generic
Thank you for your sharing. I am worried that I lack creative ideas. It is your article that makes me full of hope. Thank you. But, I have a question, can you help me?
cost of azithromycin
lisinopril 10mg tablets
lisinopril brand
otc lisinopril
buy zestoretic online
prinivil cost
tadalafil 5mg costs
buy lisinopril 2.5 mg
cheapest price for synthroid
buy cheap synthroid
where can you buy prednisone
synthroid for sale online
how to get synthroid
lisinopril cost
synthroid 0.175
1000 mg zithromax online
metformin 7267
synthroid otc
purchase lisinopril 10 mg
can i buy azithromycin over the counter in australia
zithromax z pack
zestril 10 mg
how to buy prednisone online
lisinopril online purchase
synthroid tabs 50mcg
synthroid rx cost
lisinopril 2mg tablet
where can i buy prednisone online
best price for synthroid 75 mcg
metformin 2017
order azithromycin 500mg
buy azithromycin cheap online
azithromycin 500 mg generic
synthroid costs uk
synthroid 50 pill
prednisone 10mg
synthroid 125 mcg price
prednisone cost 5mg
lisinopril 20 mg tablet
can you buy azithromycin over the counter in australia
synthroid 100
cost for 40 mg lisinopril
tadalafil rx
tadalafil uk generic
metformin 850 mg for sale
synthroid 250
lisinopril 5mg pill
synthroid coupon
order prednisone 10mg
prednisone 16 mg
synthroid brand name
buy zithromax canada
prednisone otc
10 mg prednisone tablets
how much is lisinopril 20 mg
metformin tablets where to buy
synthroid 88 mcg coupon
metformin 500 pill
zestoretic 20 25 mg
50 mcg synthroid
order azithromycin online
geinoutime.com
눈보라 속에서 젊은 왕세자는 마음에 형용할 수 없는 감정을 느꼈습니다.
synthroid cost canada
tadalafil 40 mg cheap
prednisone tablets 2.5 mg
synthroid 125 mcg
synthroid 100 mcg
purchase azithromycin online
30 mg tadalafil
azithromycin brand name in usa
synthroid 0.50 mg
tadalafil generic us
synthroid 75 pill
prednisone 20 mg over the counter
zithromax over the counter uk
prednisone 300 mg
cheap generic prednisone
tadalafil generic mexico
azithromycin 600
tadalafil tablet buy online
synthroid 25 pill
order prednisone 10mg
synthroid generic price
tadalafil tablets india online
prednisone 54899
synthroid brand 0.15mg
price of synthroid 0.125
lisinopril tabs 10mg
prednisone 50 mg coupon
120 mg prednisone
lisinopril for sale online
average cost of zithromax
tadalafil tablets sale
zestril 20 mg price
cost of zithromax 500 mg
synthroid buy
can you purchase azithromycin online
synthroid 75 mcg price in india
prednisone 10 mg brand name
can i buy 10mg prednisone over the counter
cost for 20 mg lisinopril
tadalafil tablets 20 mg cost
prednisone 20 mg
cost 50mg prednisone tablets
cost of 2.5mg prednisone
can i buy zithromax over the counter
synthroid united states
azithromycin 3080
Выбор кованого забора – это не только вопрос безопасности, но и эстетики. На a-kovka.ru мне удалось найти именно то, что я искал: уникальные дизайны и превосходное качество металла. Компания предоставляет услуги по всей Московской области, включая бесплатный замер и помощь в создании дизайна, что сделало процесс установки забора максимально удобным. Работы выполнены на высшем уровне, и теперь кованый забор является настоящим украшением моего дома.
Добро пожаловать в кузницу “А-ковка” кованые перила – ваш надежный партнер в создании красивых и функциональных перил для вашего дома. Мы находимся в Москве, всего в 91 километре от МКАД, и готовы предложить вам широкий выбор кованых изделий, выполненных опытными мастерами.
Наша цена доступна для любого покупателя, а качество наших изделий всегда остается на высоте. Мы используем современное оборудование и материалы высокого качества, чтобы каждый заказчик остался доволен результатом. Кованые перила не только придают вашему интерьеру изысканный вид, но и являются прочным и долговечным решением для вашего дома. Закажите перила в нашей кузнице и убедитесь сами в высоком качестве наших изделий!
tadalafil online 5mg
lisinopril 12.5 tablet
buy lisinopril 20 mg online uk
prinivil 10 mg
azithromycin 100mg
tadalafil 100mg india
synthroid 125
zithromax generic usa
zestril 10 mg in india
synthroid 1
where to get synthroid
tadalafil 10mg price
prinivil 10 mg tab
lisinopril 3760
50mg lisinopril
60 mg tadalafil
lisinopril 20 25 mg tab
lisinopril cost
tadalafil generic lowest price
buy lisinopril 5mg
sildenafil price
prednisone tablets 5mg price
buying zithromax in mexico
cheap generic prednisone
lisinopril 2.5
buying prednisone on line
azithromycin 250mg tablets cost
azithromycin 500 mg tablets
synthroid 150 mg cost
prednisone steroid
azithromycin 500 mg tablets cost
zithromax strep throat
buy tadalafil 20
I am not very excellent with English but I come up this very easy to translate.
prednisone 4 tablets daily
Казино Зенит zenitbet1.com
По поиску зеркало зенитбет на сегодня вы на верном пути. Зеркало официального сайта Zenitbet легко осуществляет работу на территории РФ и в полном объеме безопасно. Вы можете без опаски вписывать свои данные и быть убеждены в том, что данные не могут быть использованы другими личностями. Также средства на вашем счету находятся под защитой. Удобство в том, что сайт совпадает официальному и Вам не нужно будет привыкать к иной картинке. А также не нужно проходить вторичную регистрацию, если вы уже были зарегистрированы. В зеркале хранятся Ваши пароли, вводите их и заходите в свой кошелек.
lisinopril 20 mg tab price
tadalafil generic canada
[url=http://lisinoprill.com/]zestril canada[/url]
prednisone 10mg tablet cost
how to get metformin online
prednisone 10 mg canada
synthroid 10 mcg
БК Зенит для андроид zenitbet1.com
Если Вы искали бк зенит цупис в сети интернет, то переходите на наш веб ресурс уже сейчас. Зеркало, чаще всего, регулярно блокируют и необходимо его искать заново. С помощью сайта zenitbet1.com больше не будет сложности в поиске. Мы каждый день проверяем и обновляем ссылку на вход зеркало ЗенитБет. Можно подписаться на отправку и Вам на Email будет приходить свежая информация о входе на сайт.
generic zithromax over the counter
synthroid brand name
k8 パチンコ
非常に有意義な内容でした。このブログは本当に宝物です。
metformin over the counter usa
azithromycin pack
purchase synthroid
synthroid nz
how can i order prednisone
medication lisinopril 20 mg
zithromax for sale
prednisone 10mg tablet cost
cost of synthroid mexico
can i buy lisinopril over the counter in mexico
order tadalafil canada
synthroid 5mg
lisinopril 20 mg india
best price tadalafil online
synthroid pill
prednisone 1.25 mg
prednisone 10 mg order online
prednisone 105
tadalafil 100mg india
lisinopril 2.5 mg tablet
cheapest synthroid prices
lisinopril tabs
zestril discount
tadalafil 5mg price india
how much is prednisone 10 mg
cheap prednisone
glucophage xr generic
prednisone 200 mg
Very clear web site, thankyou for this post.
lisinopril price in india
prednisone 4mg
zestril online
Недавно я обращался в сервисный центр техники Aeg ремонт посудомоечных машин аег для ремонта своей стиральной машины. Меня приятно удивил высокий уровень сервиса и компетентность сотрудников центра. Специалисты оперативно выявили неисправность и справились с ремонтом в кратчайшие сроки. Цены на услуги вполне приемлемые, при этом предоставляется гарантия на ремонт, что внушает доверие. Советую этот сервисный центр всем владельцам техники Aeg.
how to buy prednisone
cheap online tadalafil
canadian pharmaceuticals online cheap
cost of generic lisinopril
azithromycin 100mg tablet
generic lisinopril online
average cost of prednisone 20 mg
otc prednisone
synthroid 112 cost
tadalafil 5mg price india
best price for tadalafil tablets
tadalafil 10mg australia
tadalafil professional
synthroid 0.025 mg
generic tadalafil for sale
tadalafil cost uk
taking sildenafil
best online tadalafil
can you buy synthroid over the counter
5mg tadalafil daily
generic zestril
prednisone corticosteroid
lisinopril 2019
prednisone australia
zestril coupon
lisinopril 5 mg
tadalafil online 10mg
drug prices lisinopril
synthroid 15 mg
zestril 5mg
prednisone 20mg cheap
cost of generic zithromax
tadalafil price in south africa
prinivil drug cost
zithromax 500 mg lowest price drugstore online
azithromycin otc online
average cost of zithromax
preddisone no
lisinopril pill 10mg
prinivil tabs
lisinopril 420
20 mg tadalafil
buy lisinopril 5 mg
zithromax capsules australia
tadalafil 30 mg
prednisone price canada
lisinopril 0.5 mg
metformin 1 mg
metformin tablet
generic zithromax azithromycin
lisinopril 40 mg generic
top 10 pharmacies in india
1g azithromycin cost
best tadalafil generic
can i order lisinopril over the counter
azithromycin 600
zestril 10 mg
zithromax z-pak
azithromycin canada price
buy azithromycin india
buy azithromycin australia
lisinopril
tadalafil generic otc
where to buy tadalafil in usa
where can i buy metformin over the counter
buy lisinopril 20 mg online uk
can i buy azithromycin online
azithromycin over the counter usa
cost of generic zithromax
azithromycin 250 mg pill
metformin online australia
cipla tadalafil
metformin for sale in usa
lisinopril 12.5 mg tablets
metformin buy usa
happy family store
azithromycin online sale
143 metformin
price for 125mcg synthroid
azithromycin 100 mg sale
uk azithromycin over the counter
synthroid 150 pill
lisinopril 20 mg purchase
buy synthroid online from canada
online drugstore metformin
synthroid 112 mcg prices
buy metformin online canada
zithromax 200mg
cheapest tadalafil us
metformin online usa
prinivil brand name
[url=https://lisinoprilgp.online/]lisinopril best price[/url]
azithromycin 900 mg
lisinopril 1 mg
glucophage sale
zestril 5 mg
synthroid 88 price
buy synthroid cheap
cheap metaformin
azithromycin 100 mg sale
synthroid brand name price
tadalafil 2.5 mg in india
tadalafil capsules for sale
prednisone 50 mg prices
[url=http://synthroidsl.online/]synthroid lowest prices[/url]
metformin tablet price
buy synthroid cheap
prednisone 10mg for sale
prednisone 10 mg price
prinivil 10 mg tab
lisinopril 5 mg prices
azithromycin zithromax
best tadalafil brand in india
lisinopril 2.5 mg price
tadalafil 2.5 mg online india
tadalafil tablets cost in india
happy family medical store
cost of synthroid 125 mcg
synthroid 100 mcg
azithromycin over the counter south africa
prednisone 20 mg generic
synthroid 100 mcg daily
lisinopril 10 mg tablet
synthroid canada price
express scripts com pharmacies
synthroid 150
tadalafil soft tabs
buy metformin 500mg
synthroid 088 mg
zestril
2.5 mg prednisone daily
tadalafil online mexico
buy lisinopril canada
synthroid 50 mcg cost
metformin from india
synthroid 112
prednisone 20mg buy online
metformin xr 500mg
can i buy synthroid from canada
5mg tadalafil online
synthroid 188 mcg
glucophage 1000 mg
20 mg prednisone daily
synthroid 0.05mg tablet
buying zithromax in mexico
synthroid 50 mcg coupon
prednisone 5052
purchase prednisone from india
cost of metformin in mexico
lisinopril drug
geinoutime.com
Liu Jin은 슬픔과 분노로 말했습니다. “할 수 없다면 우리는 죽을 것입니다. 우리는 하늘에 희생하기 위해 온 가족을 죽일 것입니다!”
synthroid 250 mcg
metformin 500 mg
price of zithromax
lisinopril 40 mg price
lisinopril 30 mg daily
zithromax 250 mg tab
zestril 20 mg cost
1 mg prednisone cost
Дешевые проститутки devkiru.com
Если Вы искали интим девушки в Мск, то скорее переходите на наш сайт. Мы предлагаем заказать самых дешевых проституток в Мск. Но в данном вопросе, низкая цена не означает качество. Просто у девочек в этой группе не так много практики, и принимают они в квартирах чуть далее от центра и не очень роскошных. Не нужно переживать, что невысокая цена может подпортить Ваш отдых, точнее — напротив. Вероятность великолепно провести свой отдых по выгодной стоимости-вдвойне приятнее.
prednisone 5084
prednisone 54899
cost of synthroid 75 mcg
prinivil 10 mg tab
synthroid 150 mcg coupon
tadalafil online uk
azithromycin in usa
price of lisinopril 5mg
synthroid 0.0125 online
prednisone 120 mg daily
prednisone medication
buy azithromycin australia
metformin 1000 mg
azithromycin for sale canada
where can i buy azithromycin 250 mg
synthroid 1.25 mg
purchase zithromax
synthroid 75 mg cost
prednisone 20 mg tablets coupon
how much is prednisone
can i buy prednisone over the counter in usa
metformin brand name australia
2 lisinopril
where can i get metformin
happy family rx
6 prednisone
synthroid 75 mcg tablet price
buy zithromax canada
zithromax over the counter uk
prinivil 10 mg tablet
prednisone 4mg
where can i buy generic zithromax
generic for synthroid
prednisone pill 10 mg
azithromycin over the counter nz
synthroid canada
prednisone from india
lisinopril 10 mg online
90 lisinopril
generic for zestril
prednisone 20 mg price india
how much is azithromycin
lisinopril 12.5 mg 10 mg
price for 15 prednisone
tadalafil generic price in india
tadalafil 5 mg tablet price
zestril 10 mg tablet
where can i buy prednisone online
synthroid 175 mcg
azithromycin 500
prinivil coupon
synthroid 137 mcg tab
synthroid 60 mcg
metformin online india
prednisone 2
synthroid 88 mcg tablet
synthroid 125 mg
tadalafil price comparison
zithromax in usa
azithromycin 500mg coupon
tadalafil 2.5 mg tablets
best online generic tadalafil
tadalafil cost canada
buy prednisone online nz
medication prednisone
cheap metaformin
synthroid 0.2 mg
azithromycin 500 mg tablet brand name
584 metformin
prednisone online india
lisinopril 80mg
glucophage canada online
discount zestril
zithromax in usa
tadalafil online canada
where can i get zithromax
tadalafil for sale cheap
prednisone without precription
prednisone 20mg cheap
where can i buy azithromycin
purchase zithromax
buy generic tadalafil online uk
What Is Sugar Defender?Sugar Defender is a new blood sugar-balancing formula that has been formulated using eight clinically proven ingredients that work together to balance sugar levels.
buy generic tadalafil online cheap
zithromax 500mg australia
price of prednisone in india
synthroid 0.025 mg
lisinopril 15mg
zestril drug
lisinopril 10 mg tabs
where can i buy zithromax online
azithromycin 500 tabs
cheap azithromycin 500mg
zithromax rx
prices of metformin
prednisone 5 mg pill
azithromycin in usa
Шлюхи Москвы devkiru.com
По вопросу индивидуалки царицыно Вы на правильном пути. Наш проверенный онлайн ресурс предлагает лучший отдых 18 плюс. Здесь представлены: индивидуалки, массажистки, элитные красавицы, частные интим-объявления. А еще Вы можете найти желаемую девочку по параметрам: по станции метро, по возрасту, росту, адресу, стоимости. Всё для Вашего удобства.
lisinopril 1.25 mg
prednisone no rx
tadalafil prices in india
azithromycin 100mg
zestril 40 mg
cheap azithromycin
canadian price for synthroid
can you buy azithromycin
synthroid generic cost 100 mcg
prednisone brand name canada
purchase lisinopril 10 mg
can you buy azithromycin online
synthroid 0.050 mg
glucophage australia
prednisone pill cost
levothyroxine 50 mcg
price of azithromycin 250 mg
online tadalafil canada
synthroid 200 mcg tablet
zithromax capsules buy
where to buy prednisone tablets
best price for lisinopril
tadalafil canada generic over the counter
tadalafil purchase
lisinopril 10 mg canada
10mg generic 10mg lisinopril
generic tadalafil 5mg
lisinopril 10
can you buy azithromycin online
zestril medication
lisinopril medication
cheap tadalafil online
synthroid 300 mcg canada
synthroid 150 mg
where to buy glucophage in uk
tadalafil india 10 mg
synthroid 0.1 mg daily
prednisone 50 mg
order tadalafil
buy lisinopril 10 mg online
cheapest tadalafil prices
zithromax pack
tadalafil online
prednizone for sale
metformin 1000 mg pill
predizone with out a percription
synthroid tablets price
generic synthroid prices
purchase metformin online
prednisone buy
synthroid 60 mg
tadalafil 40 mg daily
tadalafil 5mg tablets india
prednisone 40
dexamethasone 75 mg
buy amoxicillin 500mg canada
lasix uk
generic lasix
vermox usa buy
ciprofloxacin 700 mg
strattera generic price
baclofen 10 mg pill
sildenafil 100mg review
buy accutane 40 mg online
where to buy modafinil canada
dexamethasone 6 mg tablet
generic for advair diskus
buy diflucan pill
prednisone tabs
buy furosemide online usa
baclofen 10 mg tablets
modafinil best price
tretinoin 0.5 gel
vermox online uk
ciprofloxacin generic
noroxin drug
price of lasix 80 mg
where to get vermox
provigil india buy
combivent 20 100 mcg
order cheap diflucan online
sildalis tablets
trimox 500 mg
can you buy diflucan over the counter in us
tretinoin 0.4 gel
purchase lasix
ciprofloxacin 500mg capsule
synthroid 150 mcg cost
dexona tablet price in india
vermox australia online
baclofen 5 mg 1mg
toradol for headache
dexamethasone 2 mg price
buy ciprofloxacin tablets
buy cipro online paypal
dexamethasone 20 mg tablet
accutane 20 mg price in india
where can i buy bactrim
diflucan for sale online
lioresal 10mg
can you buy ventolin over the counter australia
cipro discount coupon
sildalis for sale
buy levothyroxine online
diflucan 200mg
synthroid 25 mcg cost
zithromax 500
where to buy bactrim
diflucan one
furosemide online purchase
prednisone price
where to get accutane
vermox 500mg uk
lasix iv
diflucan order online uk
azithromycin prices india
dexamethasone 5
sildalis online
toradol for kidney stones
tretinoin 05 canada
provigil 2017
purchase accutane online
baclofen 20 mg online
flomax for women
furosemide 20 mg cost
average cost of baclofen
buy ventolin online
modafinil 2019
average cost of synthroid
accutane 10mg price
zithromax for sale online
glucophage 500 mg tablet
625mg amoxicillin
[url=https://oazithromycin.online/]cost of azithromycin[/url]
generic sildenafil sale online
buy advair diskus online
5 retin a
augmentin for sale canada
flomax .4mg
online diflucan
sildenafil 20 mg how many can i take
prices bactrim
dexamethasone 0.75
toradol tablet price
bactrim 400
fluconazole without script
tamoxifen canada brand name
best over the counter lasix
bactrim tab 800 mg 160 mg
bactrim 1000 mg
how much is zithromax 500mg
baclofen 20 mg online
bactrim 800mg 160mg
retin a purchase online
prednisone 200 mg daily
how can i get azithromycin
azithromycin 250 mg over the counter
lasix medication generic
5000 mg amoxicillin
buy amoxicillin 500mg
daily baclofen
strattera 60 mg buy online
provigil 100mg
vermox online usa
tamoxifen purchase online
buy generic amoxicillin uk
accutane buy online usa
where to buy diflucan 1
Перепланировка помещений — это процесс, который включает в себя изменение конфигурации комнат, стен и перегородок. Компания “КитСтрой” предоставляет полный спектр услуг по перепланировке, начиная с проектирования и заканчивая окончательной сдачей объекта. Наши специалисты разработают индивидуальный проект, учитывая все строительные нормы и пожелания клиента. Мы гарантируем высокое качество выполнения работ и соблюдение всех необходимых стандартов.
Цель перепланировки помещений — создать удобное и функциональное пространство, отвечающее вашим потребностям.
ciprofloxacin 3
baclofen cost 20mg
buy amoxicillin 250 mg online uk
azithromycin 1mg
accutane 20 mg price
azithromycin 250 price in india
40 mg baclofen
where to buy baclofen
online retin a
can i buy provigil online
baclofen buy canada
singapore sildalis
geinoutime.com
“정말 자이모가 한 것 같다. 너무 어려서 너무 좋다.”
I haven’t checked in here for a while since I thought it was getting boring, but the last several posts are great quality so I guess I will add you back to my daily bloglist. You deserve it my friend 🙂
how to get ciprofloxacin
azithromycin tablets india
lioresal 10
where can i get provigil online
where to buy zithromax online
buy cipro on line
where can you buy zovirax
ciprofloxacin purchase
dexamethasone tablets online
vermox 500 mg tablet
where to buy modafinil uk
zithromax price in india
cost of zithromax 500 mg
diflucan online paypal
how to buy azithromycin online usa
can you buy strattera online
nolvadex cost in india
generic zithromax 250mg
cheap ventolin online
lasix 80 mg
nolvadex pct buy
tamoxifen cost nz
advair online coupon
azithromycin penicillin
diflucan cost uk
can you buy vermox over the counter
how to get zithromax over the counter
acyclovir medication over the counter
baclofen 10mg tab cost
Узаконивание перепланировки — это процесс, требующий времени и затрат. Компания “КитСтрой” предлагает услуги по узакониванию перепланировок по доступным ценам. Мы обеспечиваем полное сопровождение на всех этапах: от подготовки документов до получения разрешений. Наши специалисты знают все нюансы процесса и помогут минимизировать затраты.
Узаконивание перепланировки цена с “КитСтрой” — это выгодное и качественное решение. Обратитесь к нам для получения консультации и расчета стоимости услуг. Мы гарантируем быстрое и эффективное прохождение всех этапов узаконивания.
Холодильник Gaggenau сломался? Наш Gaggenau холодильник сервис предлагает бесплатный выезд мастера. Обращайся, и мы быстро устраним неполадки!
buy augmentin over the counter
modafinil purchase us
buy finasteride no rx
cheap ventolin uk
buy zithromax
baclofen tablet
accutane from mexico
dexamethasone 5
can i buy retin a over the counter in uk
dexamethasone 8 mg tablets
can you buy accutane online
how much is advair diskus
purchase tamoxifen
buy furesimide
order advair diskus online
azithromycin otc
azithromycin otc online
can you buy azithromycin online
metformin hcl 500mg
azithromycin for sale usa
can i buy azithromycin 500mg
cipro
tadalafil online price
vermox uk
diflucan oral
tretinoin 05 prices
average cost of tamoxifen
buy dexamethasone
buying zithromax
accutane oral
250 amoxicillin
generic for cipro
generic for zovirax
where can i buy dexamethasone
diflucan tablets buy online
price of azithromycin 250 mg
nolvadex 10mg online
glucophage sale
furosemide 40 mg coupon
dexamethasone 0.25 mg tablet
baclofen 20 mg price in india
azithromycin 500mg tablets price in india
how to get amoxicillin over the counter
accutane canada cost
buy modafinil singapore
average cost of zithromax
buy vermox uk
ciprofloxacin 50 mg
how to buy zithromax
zithromax price uk
tamoxifen cost uk
buy accutane 40 mg online
azithromycin paypal
buy cheap accutane online
lioresal 5 mg
accutane canada
azithromycin 500 mg tablet buy online
For the reason that the admin of this site is working, no uncertainty very quickly it will be renowned, due to its quality contents.
For the reason that the admin of this site is working, no uncertainty very quickly it will be renowned, due to its quality contents.
I just like the helpful information you provide in your articles
diflucan pill canada
This is really interesting, You’re a very skilled blogger. I’ve joined your feed and look forward to seeking more of your magnificent post. Also, I’ve shared your site in my social networks!
modafinil buy online us
baclofen otc uk
strattera 40 mg coupon
furosemide 20 mg coupon
This is really interesting, You’re a very skilled blogger. I’ve joined your feed and look forward to seeking more of your magnificent post. Also, I’ve shared your site in my social networks!
order provigil online canada
dexamethasone 10 mg tablet
can i buy azithromycin online usa
tamoxifen 200 mg
tadacip
diflucan medication
azithromycin 500mg australia
cipro 2016
synthroid 25 mg coupon
where can i buy modafinil
effexor price usa
6 advair diskus
toradol back pain
how to get azithromycin 500 mg
azithromycin 100mg tablets
noroxin 300
metformin
buy baclofen uk
strattera generic cost
vermox price in south africa
flomax generic brand
azithromycin 500 mg price in india
amoxicillin 500g
modafinil capsules
otc lasix
zithromax 250 mg tablet
baclofen rx
sildalis
can i buy advair online
azithromycin otc in us
how much is tretinoin in uk
generic lasix for sale
toradol 70 mg tablet
buy acutane
zithromax
order tretinoin from india
augmentin 500mg 125mg
buy acyclovir uk
modafinil 200mg buy online
vermox 100mg tablets
zithromax price
lasix 40mg tablet price
accutane india cost
buy generic advair from canada
acyclovir 792
buy zithromax
where can i buy azithromycin 500mg tablets
dexamethasone tablet 1mg
where to buy dexamethasone
albuterol brand name
cost of generic azithromycin
can you buy modafinil online
accutane 40
sildenafil for sale usa
can i buy diflucan in mexico
can i buy dexamethasone over the counter
toradol generic
dexamethasone buy online
where to get zithromax over the counter
diflucan 150 mg canada
zithromax 250mg online
cost of azithromycin in canada
sildalis canada
baclofen 5 mg
lioresal online
glucophage generic over the counter
how much is zithromax
how to get zithromax over the counter
buy ciprofloxacin 500mg online uk
amoxicillin 20 mg
zithromax 1500 mg
lasix medication over the counter
modafinil fast shipping
baclofen 10 mg buy online
where can you get accutane online
ciprofloxacin tablet brand name
where can i buy zovirax in australia
baclofen online
cost of strattera in canada
where can i get nolvadex online
where can i get accutane in australia
buy flomax generic
azithromycin 600
where can i get accutane
flomax 8
tamoxifen 20 mg 1mg
buy strattera 40 mg
1500 mg metformin
ventolin hfa 90 mcg inhaler
lasix medication over the counter
combivent respimat instructions
modafinil 2020
nolvadex 20mg price in india
furosemide 40 mg tablet cost
where to buy vermox in uk
retin a renova
buy advair online
buy azithromycin tablets in us over the counter
zithromax drug
baclofen 2
average cost of azithromycin
amoxicillin online canada
flomax cost canada
modafinil online uk
toradol nasal spray
metformin price in india
buy generic provigil online
purchase vermox
tadacip 20mg tablet
cheap vermox
dexamethasone price in usa
buy provigil india
generic zithromax 250mg
vermox otc canada
accutane price usa
baclofen 30 mg capsule
baclofen tablet generic
dexamethasone 0.75
toradol otc
flomax 4 mg cost
lioresal pill
buy provigil uk
how much is vermox
zithromax pack
diflucan 500 mg
how do i get accutane
how to get tamoxifen online
advair 50
azithromycin how to
diflucan 150 mg buy online
buy acyclovir online uk
tadacip 20mg
dexona 4mg
where to buy diflucan otc
dexamethasone 2
dexamethasone 10 mg
diflucan pill uk
diflucan in usa
cost of augmentin
where to get accutane cheap
buy retin a 1
nolvadex 10 mg tablet
cheap accutane 40 mg
can you buy zithromax online
augmentin 675 mg
strattera 60
vermox medication
sildenafil price uk
buy vermox tablets
baclofen 10 mg over the counter
advair cheapest price from india
toradol for headache
provigil discount
baclofen 40 mg
buy amoxicillin over the counter
diflucan usa
azithromycin 500 prices
tretinoin 0.2
accutane 40003395956
vermox 500
amoxicillin purchase uk
buy ventolin uk
order accutane online
how to buy azithromycin 250 mg
lasix online order
accutane price uk
azithromycin 500mg over the counter
azithromycin 250mg cost
azithromycin 500mg for sale
buy accutane online canada
generic for amoxicillin
buy baclofen 10 mg
160 mg lasix
amoxicillin usa
can you buy accutane over the counter in canada
0.009 tretinoin
buy cheap provigil
provigil online uk
tamoxifen citrate nolvadex for sale
zovirax 200 mg price
flomax 10 mg
I’m really loving the theme/design of your site. Do you ever run into any internet browser compatibility problems? A couple of my blog readers have complained about my blog not operating correctly in Explorer but looks great in Chrome. Do you have any recommendations to help fix this issue?
tretinoin retin a
buy baclofen 50mg
advair 230 21 mcg
ciprofloxacin tablet
vermox over the counter canada
diflucan online purchase
vermox tab 100 mg
best azithromycin tablet
flomax kidney stone
diflucan 50 mg price
where can i get azithromycin tablets
where can i buy provigil
dexona
advair diskus 500 mcg 50 mcg
zithromax order online
can i buy flomax
furosemide 12.5 mg tablets
lasix 20 mg price
ciprofloxacin 500 tablet price
advair cost comparison
acyclovir 30g
baclofen 2018
diflucan tablet price in india
cipro xl
where can i buy augmentin
strattera buy without rx
azithromycin 1000 for sale
buy zithromax 500mg
where to buy accutane
advair diskus discount
baclofen 10 brand name
diflucan cost in india
100mg baclofen
buy tadacip 20
dexona drug
azithromycin online sale
cipro 750 mg tablet
can you buy dexamethasone over the counter
how to buy albuterol
dexamethasone buy online
nolvadex uk cheap
buying accutane online
buy toradol tablets
order fluconazol
flomax cheap online
can i buy azithromycin over the counter in australia
modafinil canada cost
azithromycin drug
albuterol 3 mg
how to buy tadalafil online
60 mg toradol
zithromax z pak
cost cipro
provigil online cheap
dexamethasone canada
where can i get vermox
can you buy cipro online
lasix coupon
furosemide in mexico
geinoutime.com
Hongzhi 황제는 미소를 지었습니다. “당신이 실제로 나에 대해 좋은 말을 한 것은 드뭅니다.”
advair 250 50 mg
tadalafil 10 mg tablet
furosemide 40mg tabs
Недавно столкнулся с необходимостью срочного ремонта квартиры, а денег не хватало. Решил поискать варианты займов и наткнулся на телеграм-канал новые и малоизвестные МФО 2024. В канале нашёл огромный выбор новых МФО, где предлагают займы на карту без отказа и круглосуточно, даже с плохой кредитной историей. Оформил заявку, и деньги пришли на карту уже через несколько минут. Благодаря этому, я смог быстро закончить ремонт. Очень рекомендую этот канал для тех, кто ищет быстрый займ!
acyclovir tablets buy
lasix 500 mg tab
Сломался старый ноутбук, а новый срочно нужен для работы. Денег впритык, поэтому начал искать способы быстро занять средства. На телеграм-канале новые и малоизвестные МФО 2024 нашёл множество новых МФО, которые дают займы на карту без отказа. Понравилось, что можно получить деньги даже ночью и с плохой кредитной историей. Оформил заявку, деньги пришли моментально. Теперь у меня новый ноутбук и работа идёт без перебоев. Советую всем, кому нужны срочные деньги!
order vermox
azithromycin 250mg tabs
synthroid 1.25 mcg
buy vermox tablets uk
purchase azithromycin
accutane 20 mg for sale
price of cipro
cost of finasteride in india
can you buy glucophage online
vermox sale canada
canadian tadacip
order zithromax online uk
can you buy toradol over the counter
finasteride how to get
flomax buy canada
azithromycin 500mg where to buy
buy furosemide tablets uk
azithromycin 500 mg tablet price
prednisone uk buy
drug flomax generic
modafinil purchase
effexor xr 75 mg
modafinil online canada
flomax 2mg
cost ventolin australia
effexor 150 mg tablets
advair diskus from canada
diflucan 150 mg tabs
where to buy vermox
provigil medication cost
where can i get azithromycin 500 mg
Marvelous, what a webpage it is! This website gives useful data to us,
keep it up.
dexamethasone 2 mg price
dexamethasone 4 mg tablet online
buy lasix over the counter
generic provigil cost
advair cost
zithromax over the counter australia
lasix 2 mg
tadacip cost
order azithromycin 500mg
flomax capsules
zithromax europe
where to buy nolvadex
azithromycin buy online india
how to get nolvadex in canada
prednisone 5 mg tablet rx
vermox 200mg
average cost of zithromax
accutane canada cost
flomax buy online
average cost of generic zithromax
where can i get metformin online
I have recently started a website, the info you provide on this web site has helped me tremendously. Thanks for all of your time & work.
how much is the advair
metformin over the counter
where to buy bactrim
lasix 2 mg
baclofen over the counter usa
toradol otc
azithromycin 250 mg purchase
rx zithromax 600mg
provigil generic
how to get zithromax online
azithromycin in canada
metformin 250 mg tablet
modafinil for sale south africa
retin a buy online
purchase azithromycin 500 mg
acyclovir 500 mg
40 mg tadalafil
buy zithromax usa
diflucan one
generic azithromycin
Ищете надежное решение для финансовых трудностей? На нашем канале представлены новые МФО 2024, где займы доступны круглосуточно. Оформите займ от 1 до 30 рублей на 30 дней онлайн. Узнайте больше и подписывайтесь на наш канал!
zithromax capsules 500mg
furosemide 80
diflucan generic brand
where can i buy diflucan online
can you purchase zithromax
zithromax 250 mg cost
finasteride medication
azithromycin online order usa
generic ciprofloxacin 500mg
augmentin 500
zithromax generic cost
can you buy tretinoin over the counter in canada
retin a gel canada
vermox otc canada
10mg prednisone
dexamethasone 200 mg
cost of modafinil in canada
prednisone by mail
diflucan cap 150 mg
retin a micro 0.04
where can i get azithromycin 500 mg
can you buy accutane over the counter in canada
accutane capsules
diflucan 400 mg
baclofen 10 mg tabs
how much is zithromax 500mg
accutane order
accutane 5mg
buy albuterol online cheap
buy retin a india
azithromycin 1200 mg
retin a 0.05 gel
where can i get zithromax over the counter
lasix 12.5mg cost
dexamethasone 6 mg
buy provigil in mexico
advair 125 cost
baclofen price south africa
baclofen tabs 10mg
lasix 40 mg cost
lioresal cost
[url=https://albuterolo.com/]can i buy ventolin over the counter[/url]
flomax online
Ищете надежную информацию о новых МФО? Наш Telegram-канал обновляется каждый день, предлагая вам актуальные и проверенные данные. Все организации работают официально и проверены нашими специалистами. Узнайте о займы малоизвестные без отказа на карту, которые доступны всем от 18 лет. Мы поможем вам выбрать самый выгодный и удобный займ. Присоединяйтесь к нашему каналу и получайте свежую информацию каждый день!
strattera 40
Друзья, на нашем канале вы найдете уникальные предложения от новых МФО 2024. Займы от 1 до 30 рублей на 30 дней доступны всем, даже с плохой кредитной историей. Оформление быстрое и безопасное. Подписывайтесь и получайте деньги на карту без отказов!
nolvadex 10mg price
baclofen 500 mg
Ищете надежное решение для финансовых трудностей? На нашем канале представлены новые МФО 2024, где займы доступны круглосуточно. Оформите займ от 1 до 30 рублей на 30 дней онлайн. Узнайте больше и подписывайтесь на наш канал!
vermox cost canada
sildalis 120
strattera price canada
ciprofloxacin tablet price
accutane buy online
buy diflucan medicarions
furosemide price
baclofen for sale
azithromycin 40 mg
diflucan buy australia
baclofen 10 mg tablet price
baclofen rx
tretinoin 05 cost
diflucan 6 tablets
how much is vermox
zithromax singapore
dexamethasone generic brand
effexor xr 150
azithromycin 450 mg
order zithromax online uk
acytoclovir 800
baclofen 25 mg price
order fluconazole 150 mg for men
vermox tablets south africa
flomax otc usa
buy dexamethasone online
buy azithromycin 1000 mg
can you buy modafinil online
azithromycin price in mexico
buy azithromycin online cheap
sildalis in india
dexona
diflucan pill otc
where can i buy acyclovir online
order diflucan
how much is dexamethasone
ciprofloxacin 127
vardenafil research chemical
diflucan generic over the counter
azithromycin 500mg price in india
accutane 5 mg 10mg
diflucan online canada
Если у вас плохая кредитная история и вам отказывают в займе, не отчаивайтесь! Заходите в наш Telegram-канал, где мы составляем подборку новых МФО 2024 года. Мы подберем малоизвестные займы, которые дают людям с ужасной кредитной историей и просрочками до 20 000 рублей на карту в течение десяти минут. Наш канал – это ваша возможность получить деньги быстро и без отказа!
vermox canada
buy vermox in usa
Добро пожаловать в наш Telegram-канал, где мы ежедневно обновляем список новых МФО. Мы предлагаем вам самые выгодные условия для получения займов. Узнайте больше о новые мфо займы с акциями под 0%, доступных даже при плохой кредитной истории. Мы расскажем, что такое онлайн займы и как правильно ими пользоваться, чтобы избежать проблем. Подписывайтесь на наш канал и получайте деньги быстро и без отказа!
azithromycin 250 mg daily
where to get retin a gel
dexamethasone 0.25
azithromycin 250mg coupon
order azithromycin 500mg
amoxil buy
vermox over the counter uk
augmentin 457
toradol otc
buy vermox tablets uk
furosemide 40 mg tablet buy
viegra
advair 500 generic
azithromycin 25mg price
vermox 500 tablet
baclofen 5 mg
acyclovir 400 mg tablet price
nolvadex 20mg
cipro 500mg price in india
cheap provigil online
where to get vermox
how much is accutane in canada
metformin 850 mg for sale
modafinil for sale us
buy nolvadex india
tamoxifen buy usa
finasteride online bonus
how much is diflucan
buy lasix without presciption
dexamethasone price south africa
provigil india buy
dexamethasone tablets online
buy strattera online india
lasix 200
cheapest generic accutane
diflucan 15 mg
order metformin online canada
buy furesimide
order retin a gel online
where to buy vermox online
furosemide 40 mg coupon
where can i buy generic zithromax
vermox buy online europe
ciprofloxacin buy online
lasix 12.5 mg
metformin er 500 mg
sildalis 120 mg
buy metformin without a proscription
dexamethasone pill
order provigil online
order azithromycin 500mg
sildenafil tablets in india
tadacip 20 mg tablets india
acyclovir tablet singapore
diflucan generic coupon
zithromax azithromycin
accutane 1mg
can you buy accutane in mexico
where to buy retin a without a script
cost of tamoxifen 20mg tablets
diflucan 50 mg tablets
sildalis
can you buy zithromax over the counter
tamoxifen price
acyclovir 200mg
cipro online cheap
can you buy baclofen over the counter
100 mg azithromycin
how much is accutane in canada
order metformin 1000 mg
where can i get provigil online
ventolin 95mcg
dexamethasone 2 mg pill
cipro 750
lasix 100mg online
buy tretinoin australia
buy retin a canada
dexamethasone tablets 1.5 mg
canada flomax
price compare advair
generic prednisone otc
can you buy strattera online
azithromycin in usa
lasix coupon
lasix without script
cipro 500mg online
where can you buy flomax
azithromycin over the counter us
Неожиданно понадобились деньги на лечение. В таких ситуациях важно быстро найти надежный источник финансирования. Телеграм-канал Займы без процентов на карту предложил несколько вариантов займов под 0%. Оформил один из них и смог оплатить все медицинские счета.
retin a best price
amoxicillin discount
metformin hcl 1000
Моей маме исполнилось 60 лет, и я хотел сделать ей особенный подарок. Для этого потребовалась небольшая сумма, которую я нашел на новые МФО 2024 без отказа . Удивило, как быстро и легко можно получить деньги, даже с не самой лучшей кредитной историей. Подарок удался, и мама была в восторге.
azithromycin rx coupon
how can i get provigil
azithromycin 500 mg tablet price in india
where to buy modafinil canada
accutane 20 mg price in india
lioresal cost
synthroid tabs 50mcg
how to get azithromycin 1g
modafinil tablets in india
can i order azithromycin online
dexamethasone brand name
flomax capsule
zithromax buying
albuterol tablets for sale uk
generic advair diskus canada
nolvadex for sale online
zithromax tablets australia
dexamethasone cost
azithromycin tabs 250 mg
Друзья пригласили меня в поход в горы. У меня не было снаряжения, и я думал отказаться. Но вспомнил про малоизвестные МФО без отказов и нашел займ с выгодными условиями. Вскоре у меня было всё необходимое для похода, и это приключение стало одним из самых ярких в моей жизни.
90 vermox
furosemide 10 mg tablet
buy lasix online
how to purchase provigil
buy ventolin canada
cheapest price for amoxicillin
azithromycin 250 mg for sale
dexamethasone 200 mg
advair 500
accutane for sale online
azithromycin without rx
buy cheap zithromax online
cost of tamoxifen uk
buy furosemide online australia
zithromax 100
azithromycin in usa
where can i buy vermox in uk
lasix tablets price
buy vermox online usa
accutane 30 mg price
dexamethasone tablet 1mg
order lasix 40 mg
amoxicillin tablets cost
price of tamoxifen 20 mg
buying baclofen online
effexor 150 mg tablets
provigil online cheap
order vermox over the counter
buy zithromax without presc
azithromycin 250mg cost
sildalis online
where to buy azithromycin
synthroid 0.88
baclofen tab 10mg
cheap zovirax
toradol pill cost
synthroid 150
cheap albuterol online
where to buy dexamethasone
baclofen online
modafinil india online
accutane for sale online
can you buy dexamethasone over the counter
ipledge accutane
lioresal
bactrim f
sildalis cheap
dexamethasone tablets online
accutane 20 mg daily
dexamethasone for sale
tretinoin 0.05 cost
At MCI Clinic, we provide outstanding glaucoma treatment, ensuring you regain and maintain good vision. Our experienced team uses cutting-edge technology to diagnose and manage glaucoma effectively. With a range of treatments, including medications, laser therapy, and surgery, we tailor our approach to meet your specific needs.
Choosing MCI means trusting experts who prioritize your eye health and deliver top-notch care. Our commitment to using advanced methods and equipment ensures that your vision remains clear and healthy for years to come.
MCI Clinic – astigmatizm
vermox over the counter uk
metformin 1000 mg price in canada
cost of ventolin
accutane online cheap
generic baclofen tablet
order modafinil australia
purchase advair
tretinoin gel 0.05
accutane.com
generic zithromax 500mg india
dexamethasone india
cipro cost
albuterol 8.5 g
dexamethasone 4 mg cost
baclofen comparison
baclofen australia
dexamethasone 1.5 tablet
accutane online india
can you buy amoxicillin over the counter canada
zovirax tablet price
azithromycin 250mg
accutane tablets price
[url=https://dexamethasoneff.com/]dexamethasone tablets canada[/url]
advair medication
glucophage 1000 price
drug acyclovir 800 mg
accutane 5mg
modafinil tablet
diflucan drug
advair 500 diskus
albuterol 90 mcg inhaler
where to buy modafinil online
advair medication cost
zitromax
cost of accutane in canada
cost of modafinil 200mg
buy sildalis online
zithromax over the counter canada
generic diflucan 150 mg
buy ventolin australia
rx azithromycin
can you buy metformin over the counter uk
how much is furosemide 40 mg
effexor cost canada
geinoutime.com
Dowager 황후는 주위를 둘러보고 가볍게 “가까이”라고 말했습니다.
baclofen tablets brand name
1 retin a
where to purchase zithromax
azithromycin 500 mg generic
where can i get azithromycin
I am extremely impressed with your writing skills and also with the layout on your weblog.
Is this a paid theme or did you modify it yourself?
Anyway keep up the nice quality writing, it’s rare to
see a nice blog like this one these days.
It’s a pity you don’t have a donate button! I’d definitely
donate to this brilliant blog! I guess for now i’ll settle for bookmarking and adding your RSS feed to my Google account.
I look forward to new updates and will share this website with my Facebook group.
Chat soon!
Today, while I was at work, my sister stole my iPad and tested to
see if it can survive a 30 foot drop, just so she can be a
youtube sensation. My iPad is now destroyed and she has 83 views.
I know this is completely off topic but I had to share it with someone!
otc toradol
flomax for ed
modafinil online uk paypal
azithromycin 1g price
azithromycin 40 mg
toradol pain shot
azithromycin 1g online
vermox buy online uk
Does your website have a contact page? I’m having problems locating it but, I’d like to
shoot you an email. I’ve got some recommendations for
your blog you might be interested in hearing.
Either way, great blog and I look forward to
seeing it grow over time.
zithromax 600 mg tablets
buying azithromycin in mexico
buy modafinil online
where can i buy diflucan
can i buy diflucan over the counter in canada
azithromycin 250 mg otc
buy cheap diflucan online
azithromycin 500
azithromycin buy us
buy azithromycin uk
modafinil rx
When I initially commented I clicked the “Notify me when new comments are added” checkbox and now
each time a comment is added I get several emails
with the same comment. Is there any way you can remove me from that service?
Cheers!
furosemide 50 mg tablets
azithromycin 500 mg cost in india
lioresal 10 mg
lasix to buy
advair drug prices
azithromycin in mexico
generic lasix
albuterol canada
generic noroxin
acyclovir usa
dexona price
azithromycin script
where can you get modafinil
best price generic accutane
vermox usa
zithromax 500
can you diflucan over the counter
vermox 100mg tablets
buy azithromycin online usa
no script generic lasix
accutane gel
dexamethasone medication
diflucan 150 mg tablet
ciprofloxacin capsule
azithromycin 300 mg
baclofen cost uk
[url=http://amoxicillinir.online/]augmentin 675 price[/url]
augmentin for sale canada
ciprofloxacin 127
diflucan 150 mg price in india
ciprofloxacin 3
dexamethasone tablet 1mg
azithromycin 250 mg tablet price
Ищете надежное место для получения займа? Присоединяйтесь к нашему телеграм-каналу какие займы дают без отказа на карту отзывы ! У нас собраны МФО, которые выдают деньги без отказов и проверки кредитной истории. Получите первый займ под 0% до 15 000 рублей всего за 10 минут! Также в канале вы найдете списки новых МФО 2024 года, где можно получить мгновенные микрозаймы даже при плохой кредитной истории и просрочках. Вступайте и решайте свои финансовые проблемы!
zovirax 5g price
modafinil europe
provigil 200 mg coupon
zithromax 250 tablet
can you buy tadalafil over the counter
purchase augmentin online
vermox for sale
drug toradol
azithromycin tablets 250 mg
lasix 90 20mg
azithromycin tabs 250mg
prednisone 20mg online
where to get diflucan otc
how much is baclofen 10 mg
purchase azithromycin 500mg
buy accutane usa
accutane generic canada
where can i buy flomax
lasix 20 mg tabs
baclofen pill price
how to get cheap accutane
can you buy zovirax over the counter in australia
purchase amoxicillin 500mg
flomax for women urinary retention
zithromax azithromycin
flomax uk otc
cost of advair in us
dexamethasone uk
flomax over the counter uk
buy lasix online cheap
buy tretinoin online mexico
azithromycin 600 mg price
cost of azithromycin in india
modafinil online australia
azithromycin online india
accutane how to get
[url=http://azithromycinmds.com/]zithromax capsules 250mg[/url]
At MCI Clinic, we specialize in cataract treatment with extensive experience, state-of-the-art equipment, and affordable prices. Our skilled professionals perform advanced procedures such as phacoemulsification, ensuring precise removal of the cloudy lens and its replacement with a high-quality artificial one. The surgery is quick, safe, and minimally invasive, providing excellent outcomes for our patients.
Choosing MCI means benefiting from top-tier medical care without the high cost. We are committed to restoring your clear vision and improving your quality of life through effective, cost-efficient cataract treatments.
MCI Clinic – лечение глаукомы
baclofen 10mg tablets
vermox from mexico
At MCI Clinic, we specialize in cataract treatment with extensive experience, state-of-the-art equipment, and affordable prices. Our skilled professionals perform advanced procedures such as phacoemulsification, ensuring precise removal of the cloudy lens and its replacement with a high-quality artificial one. The surgery is quick, safe, and minimally invasive, providing excellent outcomes for our patients.
Choosing MCI means benefiting from top-tier medical care without the high cost. We are committed to restoring your clear vision and improving your quality of life through effective, cost-efficient cataract treatments.
MCI Clinic – tratamentul astigmatism
vermox over the counter canada
lioresal medication
order zithromax online canada
cost baclofen
generic lioresal
baclofen 10 mg tablet online
flomax liquid
Лаборатория труда соут safetysystemsgroup.com
Организация Safety Systems проводит специальную оценку условий труда на любом предприятии. Наш главный офис расположен в Москве, но также в большинстве городов России у нас есть филиалы. Проверка проводится в обязательном порядке для всех компаний, чтобы снабдить безопасность для работников и убавить вероятность на приобретение штрафов.
По поводу соут москва организации заходите на наш сайт. Оценочные события должны осуществляться в организациях не менее, чем раз в 5 лет. Но еще у особых отраслей есть собственные сроки. Непременно ознакомьтесь с тем, что нужно конкретно Вам на сайте safetysystemsgroup.com уже сейчас.
Ищете способ быстро получить деньги? Подпишитесь на наш телеграм-канал микрозаймы всем ! Здесь мы собрали лучшие МФО, которые выдают деньги без отказов и проверки кредитной истории. Первый займ под 0% до 15 000 рублей всего за 10 минут! В канале также есть подборки новых МФО 2024 года, выдающих микрозаймы мгновенно, даже если у вас плохая кредитная история или просрочки. Присоединяйтесь и решайте финансовые вопросы легко!
strattera price
furosemide 30 mg
Хотите получить деньги быстро и без лишних вопросов? Подпишитесь на телеграм-канал займ который дают всем ! У нас вы найдете МФО, выдающих деньги без отказов и проверки кредитной истории. Первый займ под 0% до 15 000 рублей всего за 10 минут! Также в канале есть списки новых МФО 2024 года, которые дают мгновенные микрозаймы даже с плохой кредитной историей и просрочками. Присоединяйтесь и забудьте о финансовых проблемах!
dexamethasone tablets online
buy vermox online nz
ventolin albuterol
tadalafil gel
order vermox
accutane 40
can you buy zithromax over the counter in australia
buy generic azithromycin
buy strattera uk
lasix tablets
effexor 225 mg tablet
1600 mg acyclovir
diflucan otc
azithromycin over the counter uk
furosemide in canada
azithromycin 500 price in india
tamoxifen gynecomastia
2019 advair coupon
price of advair
accutane us
can you buy baclofen over the counter us
cipro discount
metformin pill for sale
where can i buy azithromycin 250 mg
I pay a visit everyday a few blogs and information sites to read articles, but
this web site provides feature based posts.
toradol buy
advair buy
where to buy cipro
purchase advair online
buy furesimide online
metformin 100 tablet
Greetings! Very useful advice within this article!
It is the little changes that will make the biggest changes.
Many thanks for sharing!
zovirax tablets canada
diflucan from india
metformin 850 mg price
tretinoin 05 coupon
buy online zithromax
[url=http://dezithromax.online/]zithromax tablets online[/url]
diflucan online
modafinil 50mg
deltasone generic 5mg
bactrim online no prescrition
azithromycin buy online
where to buy accutane uk
buy generic flomax online
can i buy provigil in mexico
buy azithromycin 250mg online
dexamethasone 1
albuterol 90 mcg coupon
azithromycin 250 mg coupon
azithromycin 250 price
where can you buy nolvadex
where to get nolvadex
diflucan brand name in india
retin a 08
vermox sale
accutane online canada
azithromycin tablet price
where can i get prednisone
azithromycin cost
metformin brand name us
azithromycin 2017
I really like your blog.. very nice colors & theme.
Did you design this website yourself or did you hire someone
to do it for you? Plz respond as I’m looking to create my own blog and would
like to know where u got this from. thank you
accutane cost australia
accutane australia online
dexamethasone over the counter
azithromycin for sale online
dexamethasone 8 mg
cheap azithromycin online
generic modafinil price
ciprofloxacin 500mg capsule
best retin a
combivent aer respimat
azithromycin 600 mg tablet
how can i get provigil
buy cheap cipro online
where to purchase modafinil
cipro 250 mg coupon
accutane in india
baclofen price uk
generic effexor xr
advair 500
30 mg baclofen
16 mg dexamethasone
buy baclofen usa
modafinil europe
where to get flomax
accutane online no rx
canada azithromycin over the counter
furosemide 10 mg tablet
azithromycin otc usa
purchase azithromycin 1g
buy sildalis 120 mg
baclofen 420 mg
This text is priceless. Where can I find out more?
lowest price for advair
zithromax capsules buy
cheap albuterol inhalers
dexona 8mg tablet
furosemide uk buy
order ciprofloxacin online
order advair diskus online
cheap generic amoxicillin
order zithromax uk
buy provigil online usa
retin a where to buy uk
dexamethasone tablets 1.5 mg
metformin price canada
dexona 4mg tablet
generic advair diskus
advair 250/50
zovirax 5 ointment
azithromycin price in india
buy fluconazole online
buy flomax otc
provigil nz
cost of albuterol
diflucan drug
accutane prices
toradol 12.5
zitromax
diflucan 150 cost
buy baclofen canada
where can i buy azithromycin
20mg nolvadex daily
where can you buy azithromycin in australia
buy baclofen
buy azithromycin canada
geinoutime.com
그 불은 집을 태웠지만 내 돈이기도 했다.
buying amoxicillin in canada
generic lioresal
diflucan buy online
retin a 0.08 coupon
flomax over the counter medication
azithromycin 500 tablet
amoxicillin price uk
lasix online
Useful information. Lucky me I discovered your web site accidentally, and I am stunned
why this coincidence did not happened in advance! I bookmarked it.
baclofen tab 10mg
zithromax 250 mg tablet price
furosemide 4
Преимущества теневого плинтуса в декорировании помещения,
Как правильно установить теневой плинтус своими руками,
Как использовать теневой плинтус для создания уникального интерьера,
Ретро-стиль с использованием теневых плинтусов: идеи для вдохновения,
Как подобрать цвет теневого плинтуса к отделке стен,
Как спрятать коммуникации с помощью теневого плинтуса: практические советы,
Преимущества использования теневого плинтуса с интегрированной подсветкой,
Современные тренды в использовании теневого плинтуса для уюта и красоты,
Почему теневой плинтус – важная деталь в оформлении интерьера
плинтуса напольные плинтуса напольные .
Преимущества теневого плинтуса в декорировании помещения,
Шаг за шагом инструкция по установке теневого плинтуса,
Как использовать теневой плинтус для создания уникального интерьера,
Модные тренды в выборе теневых плинтусов для современного дома,
Гармония оттенков: выбор цвета теневого плинтуса для любого интерьера,
Как спрятать коммуникации с помощью теневого плинтуса: практические советы,
Интересные решения с теневым плинтусом и подсветкой: идеи для вдохновения,
Современные тренды в использовании теневого плинтуса для уюта и красоты,
Почему теневой плинтус – важная деталь в оформлении интерьера
высота плинтуса https://plintus-tenevoj-aljuminievyj-msk.ru/ .
sildalis 120
Микрозаймы – отличное решение для тех, у кого проблемы с кредитной историей. В Telegram-канале Займы с плохой КИ мы собрали лучшие микрозаймы, доступные даже при плохой кредитной истории. Быстро, удобно и без лишних отказов! Подпишитесь на наш канал и получите займ уже сегодня!
lowest price for advair
generic for zithromax
lasix 500
where to purchase accutane
Если у вас испорченная кредитная история, это не конец света! В нашем Telegram-канале Займы с плохой КИ мы предлагаем вам актуальные займы от проверенных кредиторов. Получите необходимую сумму быстро и без лишних проверок. Подпишитесь на канал и найдите лучший вариант для себя!
baclofen 10 mg tablet
zithromax
dexamethasone 10 mg
buy azithromycin us
finasteride proscar
cheap amoxicillin 500mg online
ciprofloxacin otc
buy tadacip 10
azithromycin 100mg
accutane 40 mg online
azithromycin 500 mg tablet buy online
buy lasix over the counter
can you buy azithromycin online
vermox cost
buy baclofen india
diflucan uk online
how to get accutane in canada
over the counter medication flomax
buy generic azithromycin
lioresal drug
azithromycin 1mg
azithromycin 2019
ciprofloxacin 750 mg
ciprofloxacin over the counter
baclofen 25 mg
advair diskus 250 cost
diflucan tablet india
dexamethasone 200 mg
flomax 0.4mg price
can you purchase diflucan over the counter
flomax price comparison
average cost of zithromax
advair uk
vermox uk
Hey! I know this is kind of off topic but I was wondering which blog
platform are you using for this site? I’m getting sick and
tired of WordPress because I’ve had issues with hackers and I’m looking at alternatives for another platform.
I would be great if you could point me in the
direction of a good platform.
buy accutane online usa
where can i buy zovirax in australia
furosemide 120 mg daily
how to buy diflucan
vermox over the counter usa
tretinoin 0.25mg
azithromycin buy over the counter uk
tamoxifen buy australia
azithromycin price
buy furosemide tablets online uk
lasix cheap
generic advair diskus canada
dexamethasone 2mg tablets
Добро пожаловать на наш сайт о продаже недвижимости! Здесь вы найдете полезные статьи, советы и новости о рынке недвижимости, юридических аспектах покупки и продажи недвижимого имущества, аренде коммерческих помещений, налогах на недвижимость и многом другом.
https://glavdecor-ekb.ru/
best accutane brand
diflucan online canada
strattera 60
buying retin a online
ciprofloxacin price uk
buy vermox
zithromax in usa
Хотите быть в курсе всех актуальных тенденций на рынке недвижимости? На нашем ресурсе вы найдете полезные статьи о стоимости аренды квартир, ценах на жилье, займах под залог недвижимости.
Узнавайте первыми о самых выгодных предложениях от экспертов, чтобы сделать правильный выбор и сэкономить свои деньги.
https://ucnedv.ru/
baclofen 10 mg tablet price in india
where to get diflucan over the counter
modafinil over the counter
accutane 20 mg
[url=http://lasixor.online/]furosemide 40 mg cost[/url]
albuterol inhaler 90 mcg
bactrim otc
flomax discount
cipro 500mg cost
medication advair diskus
advair 15
cipro mexico
geo peptides tadalafil
buy ventolin over the counter
otc synthroid
generic provigil cost
flomax cost comparison
buy sildalis online
80 mg accutane
baclofen 10 mg tab
baclofen
noroxin drug
baclofen tablets
Nice post. I was checking constantly this weblog and I’m inspired!
Extremely helpful information particularly
the last part 🙂 I maintain such information much. I used to be looking for
this certain information for a very lengthy time.
Thank you and best of luck.
advair diskus price canada
Незаменимая часть гардероба – тактичные штаны, подчеркнут ваш стиль.
Отличный выбор для походов и путешествий, тактичные штаны подарят вам удобство и защиту.
Надежный пошив и долговечность, сделают тактичные штаны незаменимым атрибутом вашего образа.
Современный стиль и практичность, подчеркнут вашу индивидуальность и статус.
Неотъемлемый атрибут современного мужчины – тактичные штаны, которые подчеркнут вашу силу и уверенность.
тактичні штани зимові https://taktichmishtanu.kiev.ua/ .
sildalis online
Канализация на участок Екатеринбург neseptik.com
По запросу бак для канализации установка мы Вам непременно окажем помощь. Сейчас выдающимся запросом пользуются загородные дома, дачи, коттеджи. Люди как будто измотались от социальной жизни и все гонятся к уединению и комфортной обстановке за городом. Но на фазе выбора и покупки участка, лучше учесть очень многие нюансы, среди которых вопрос с канализацией. Если Вы придете к нам перед стройкой, то это будет одним из самых верных решений в Вашей жизни!
Excellent post. Keep posting such kind of information on your site.
Im really impressed by it.
Hello there, You’ve done an incredible job. I’ll definitely digg
it and individually suggest to my friends. I’m confident they will be benefited from this website.
baclofen 25 mg tablet
lasix tablet
cheap provigil canada
lasix 40 mg price in india
can you buy nolvadex over the counter
tretinoin 0025
cheap diflucan online
combivent respimat pi
accutane 80 mg daily
geinoutime.com
이때 개인의 고충을 신경 쓸 때가 아니다.
baclofen 100mg price
buy generic accutane 40 mg
Hi, i think that i saw you visited my weblog so i came to “return the favor”.I am trying to find things to enhance my website!I suppose its ok to use a few of your ideas!!
diflucan online india
zithromax 500 mg
Узнайте все о покупке квартир от надежного застройщика, получении выписки из госреестра недвижимости, получении кредитов под залог и налоговом вычете за покупку жилья на нашем сайте!
Актуальные и информативные статьи помогут вам разобраться во всех нюансах рынка недвижимости и сделать обоснованный выбор.
https://donskoy-alians.ru/
retin a 1 cost
Узнайте все о покупке квартир от надежного застройщика, расчетах налогов на недвижимость, получении кредитов под залог и налоговом вычете за покупку квартиры на нашем сайте!
Актуальные и информативные статьи помогут вам разобраться во всех вопросах рынка недвижимости и сделать правильный выбор.
https://donskoy-alians.ru/
diflucan discount
buy albuterol online canada
Heya this is kind of of off topic but I was wondering if blogs use WYSIWYG
editors or if you have to manually code with HTML. I’m starting a blog soon but have no coding skills so I wanted to get advice from
someone with experience. Any help would be greatly appreciated!
azithromycin 500 mg over the counter
zithromax 500 mg
can you buy amoxicillin over the counter in usa
advair diskus coupon
retin a buy online india
Подземная канализация купить neseptik.com
Что касается – емкость для воды септика мы Вам непременно окажем помощь. Сейчас выдающимся спросом пользуются частные дома, дачи, таунхаусы. Жители как будто измотались от социальной жизни и все стремятся к природе и комфортной обстановке за городом. Но на стадии выбора и покупки участка, рекомендуем учесть очень необходимые моменты, в том числе вопрос с септиком. Если Вы обратитесь к нам перед застройкой, то это будет одним из лучших выборов в Вашей жизни!
lasixs water pill
advair diskus 100
buy cheap modafinil
trimox price
how to get accutane australia
Заказать бак металлический для канализации neseptik.com
Приобрести достойный септик можно кликнув на страницу – бак под канализацию купить прямо сейчас. Звоните по телефону +7(902)871-48-01 и мы ответим на любые ваши вопросы. Находимся по адресу: г. Екатеринбург, ул. Вилонова, д. 33. Время работы с пн по пт с 8:00 до 19:00. Звоните, приезжайте, мы будем рады сотрудничать с Вами!
nolvadex tab 1mg
Keep working ,terrific job!
order provigil online canada
buy amoxil online australia
amoxicillin pill
where to buy modafinil over the counter
tamoxifen 5 mg
dexamethasone buy online uk
buy finasteride online 5mg
tretinoin capsules 10mg
where can i buy lasix online
flomax 400 mcg
vermox tablet india
price of 21 acyclovir
azithromycin online canada
can i buy flomax
buy vermox
zovirax canada
azithromycin tablets
azithromycin buy online
where to get nolvadex
dexamethasone cost
ciprofloxacin 500 mg capsules
strattera drug
tretinoin price in mexico
furosemide costs
over the counter baclofen
baclofen tab 20mg
sildenafil buy over the counter
ventolin 200 mg
order cheap diflucan online
where can i buy azithromycin
cheap albuterol online
azithromycin 500 mg tablet brand name
azithromycin for sale australia
What is ProNerve 6? ProNerve 6 is a doctor-formulated nutritional supplement specifically marketed to individuals struggling with nerve pain.
tretinoin price canada
diflucan 50
buy azithromycin over the counter uk
buy zithromax azithromycin
how to buy accutane online
azithromycin 500 mg tabs
azithromycin price
advair 115 21 mcg
furosemide 40mg tabs
azithromycin for sale australia
where can i get zovirax
can i buy azithromycin over the counter uk
where to get vermox
ciprofloxacin
ventolin 2018
furosemide drug
can you buy advair over the counter
order difucan
strattera cost
accutane buy
price of diflucan in india
baclofen australia
provigil purchase
azithromycin cheapest price
[url=http://glucophage.online/]metformin tablet 500mg price[/url]
buy flomax
amoxicillin 3109
accutane price in usa
zithromax no rx
azithromycin 787
amoxicillin 500 mg coupon
cheap baclofen uk
can i buy flomax
vermox 500mg tablet
buy zithromax cheap
acyclovir 200mg
zithromax coupon
diflucan tabs
generic cipro
baclofen comparison
azithromycin cap 500 mg
diflucan online canada
strattera online india
order modafinil online usa
how much is a diflucan pill
buy generic advair online
tamoxifen uk price
buy acyclovir
prednisone 5092
cost of modafinil in usa
how to get advair cheap
buy cheap zithromax online
diflucan drug coupon
furosemide brand name uk
albuterol for sale usa
ciprofloxacin over the counter uk
vermox drug
zithromax 1000mg
generic azithromycin
dexamethasone 0.5 mg tablet
albuterol buy online
accutane otc drug
azithromycin india
buy accutane uk
generic zithromax online
azithromycin tablets 250 mg price in india
baclofen 5 mg tablet price
buy azithromycin over the counter
zithromax drug
azithromycin medication
dexamethasone pill
diflucan candida
zithromax tablet
azithromycin
baclofen australia
dexamethasone 0.5 mg tablet
fluconazole diflucan
price of accutane in south africa
augmentin 1g
baclofen no preciption
diflucan 150
can i buy furosemide online
strattera generic
provigil 400 mg
accutane tablets online
diflucan price australia
how to buy modafinil australia
can i buy zovirax over the counter in canada
[url=http://avermox.online/]vermox in canada[/url]
how can i get accutane
dexamethasone otc
bactrim ds 800 160
lasix 80
Wow, marvelous weblog format! How long have you ever been running a blog for? you made blogging look easy. The full look of your site is fantastic, let alone the content material!
production company Venice Italy
azithromycin cost price
finasteride 1mg coupon
tretinoin capsule brand name
diflucan coupon canada
sildenafil 120
zovirax 200mg tablets price in india
accutane online canada
diflucan price singapore
vermox over the counter usa
bactrim 1600
zithromax online
dexamethasone 4 mg tablet brand name
best generic accutane
synthroid 0.88
order vermox online
nolvadex tablets india
can you purchase diflucan over the counter
how to get flomax
Superb site you have here but I was wondering if you knew of any community forums that cover the same topics talked about here? I’d really like to be a part of group where I can get advice from other experienced individuals that share the same interest. If you have any suggestions, please let me know. Appreciate it!
lasix 40 mg price
Установка крыши на балконы спб specbalkon.ru
Что касается замена фасадного остекления спб на выгодных условиях, приходите к нам. Контактный телефон +7(812)240-94-42 или закажите обратный звонок на вышеуказанном сайте. Мы осуществляем монтаж в точно обговоренный срок, обычно в течение 1-3 дней. Даётся гарантия на изделия в среднем 5 лет, на монтаж — 3 года. Оплата осуществляется по факту исполненных работ, предоплата не нужна.
glucophage 500mg buy online
accutane 20 mg buy online
albuterol mdi inhaler
azithromycin in canada
dexamethasone drug
over the counter flomax
otc albuterol
dexamethasone generic brand
flomax in usa
flomax erectile dysfunction
dexamethasone otc
generic azithromycin cost
furosemide 60 mg tablets
azithromycin buy online nz
furosemide 3170
where to buy zithromax over the counter
cheap azithromycin online
bactrim 800 150 mg
prednisone price australia
I read this paragraph fully about the comparison of most recent and previous technologies, it’s awesome article.
flomax glaucoma
Heya i am for the first time here. I found this board and I to find It really useful & it helped me out much. I’m hoping to offer one thing back and help others such as you aided me.
glucophage 1000 mg price
diflucan 150 mg
[url=https://azithromycinhq.com/]zithromax brand name[/url]
Hi, constantly i used to check web site posts here early in the break of
day, since i like to find out more and more.
ciprofloxacin online uk
prednisone 10 mg tablet price
tretinoin capsules
diflucan 125mg
Hi there Dear, are you truly visiting this web site daily, if so
then you will definitely take nice knowledge.
dexamethasone 500 mg tablet
tadacip india
zithromax otc
azithromycin order online uk
zithromax online canada
lioresal sale
zithromax buy online
dexamethasone 6 tablet
where to buy finasteride
amoxicillin no script
augmentin usa
drug flomax
dexamethasone tablets 1.5 mg
buy amoxicillin 500mg canada
where to buy azithromycin over the counter
zithromax capsules 500mg
how much is retin a in mexico
azithromycin 500mg where to buy
lasix without script
When I originally commented I clicked the “Notify me when new comments are added” checkbox and now each time a comment is added I get several emails with the same comment. Is there any way you can remove me from that service? Bless you!
modafinil over the counter uk
zithromax for sale cheap
bactrim nz
toradol for headache
Остекление балконов в Санкт-Петербурге specbalkon.ru
Если Вам нужно теплое фасадное остекление балкона прямо сегодня, то мы вам непременно окажем помощь. Услуга по замене холодного фасадного остекления по теплое в данный момент очень востребована. При покупке жилья в новом доме очень часто застройщик устанавливает на балкон холодное, не очень качественное остекление, которое лучше менять сразу же после приобретения. Теплое остекление балкона имеет большое количество плюсов: окна не замерзнут даже в самые морозные зимы, на балконе возможно сделать любое пространство, цветы будут стоять при комнатной температуре, на балконе можно сделать места для хранения и вещи не деформируются. Поэтому предлагаем Вам замену остекления сделать как можно скорее и по лучшей цене.
tadacip prices
accutane india cost
metformin 52080
Псс… Хотите узнать о самых выгодных направлениях инвестирования в недвижимость, основных рисках и способах их минимизации? Читать https://aibismach.ru
Утепление балкона с фасадным остеклением specbalkon.ru
Если Вам необходимо стоечно ригельная система фасадного остекления alutech прямо сегодня, то мы вам непременно окажем помощь. Услуга по смене холодного фасадного остекления по теплое сейчас очень востребована. При покупке жилплощади в новом доме очень часто застройщик устанавливает на балкон холодное, не очень качественное остекление, которое лучше поменять сразу же после приобретения. Теплое остекление лоджии имеет большое количество плюсов: окна не замерзают даже в самые холодные зимы, на балконе можно сделать любое помещение, цветы будут стоять при комфортной температуре, на балконе можно сделать места для хранения и вещи не испортятся. Поэтому предлагаем Вам замену остекления сделать как можно быстрее и по лучшей цене.
buy acutane
vermox tablets where to buy
vermox over the counter australia
diflucan over the counter uk
where to get provigil
furosemide 40 mg buy online
vermox online
azithromycin from mexico
zovirax coupon
diflucan in usa
synthroid 1
buy ventolin over the counter with paypal
dexamethasone 80 mg
where can i get metformin online
strattera capsule
sildalis canada
baclofen 25mg
azithromycin 2000 mg
strattera 80 mg cost
azithromycin 200mg tablets
buy baclofen uk
azithromycin 500 mg tablet for sale
strattera generic capsule 25mg
best price zithromax 250mg
flomax inhaler
ciprofloxacin 500mg price
buy accutane cheap online
lasix 40 mg tablet
Hi there everyone, it’s my first visit at this web site, and post is really fruitful in favor of me, keep up posting these types of articles.
lgo4d
how much is amoxicillin 30 capsules
buy finasteride online 5mg
buy baclofen europe
advair 500 50
accutane 10mg for sale
tretinoin coupon
buy azithromycin over the counter canada
tretinoin 0.1 coupon
can i buy toradol over the counter
retin a price in india
amoxicillin tablet
where to buy diflucan in canada
ciprofloxacin 500mg cost
tadacip 40 mg
acyclovir 50mg
accutane online uk
furosemide 20 mg brand name
purchase cipro
flomax 4 mg price
zithromax z pack
geinoutime.com
“…” 분명히 Hongzhi 황제는이 사람에 대해 말한 것을 후회하기 시작했습니다.
cost of accutane
baclofen in india
augmentin 750 mg
buying provigil in mexico
online rx diflucan
advair 100 50 mg
Обучение младший медицинский персонал maps-edu.ru
Насчёт баллы нмо для медсестер – Вы на точном пути. Направления, по которым мы можем обучить: охрана труда, агрономия и сельское хозяйство, бухгалтерское дело, дефектология, пожарная безопасность, закупки, экономика и финансы, промышленность, нефтяная и газовая промышленность, метрология и стандартизация и многие другие.
fureosinomide
lasix 12.5mg cost
provigil how to get
lioresal 25 mg
buy azithromycin 1000 mg
how to order modafinil online
[url=https://modafinilmip.online/]buy provigil 100mg online[/url]
azithromycin in usa
modafinil 200mg price
flomax singapore
advair cost mexico
buy accutane uk
buy generic provigil
Псс… Интересные статьи о недвижимости. Аренда, купля/продажа, недвижимость как бизнес. Подробнее http://sma-repair.ru
zithromax purchase canada
purchase azithromycin 500mg
toradol rx
500mg amoxicillin price
lasix generic
Обучение дистанционно maps-edu.ru
По вопросу профессиональная переподготовка строительство онлайн, мы Вам непременно поможем. Звоните по контактному телефону 8(800)777-06-74 и задавайте все возникшие вопросы. Звонок по России бесплатный. Территориально расположены по адресу: г. Иркутск, ул. Степана Разина, д. 6. На онлайн ресурсе maps-edu.ru вы также сможете обратиться в службу помощи и Вас проконсультирует наш менеджер.
Учиться на логопеда дистанционно maps-edu.ru
Насчёт младший медицинский персонал обучение – Вы на точном пути. Направления, по которым мы обучаем: строительство, агрономия и сельское хозяйство, педагогика, физическая культура и спорт, юриспруденция и право, закупки, культура и искусство, документоведение и делопроизводство, нефтяная и газовая промышленность, метрология и стандартизация и многие другие.
effexor 37.5 mg tablets
ciprofloxacin 500 for sale
order amoxicillin online
Greetings! Very helpful advice in this particular post!
It is the little changes which will make the most important
changes. Thanks for sharing!
Приветствую. Может кто знает, где найти полезные статьи о недвижимости? Интересуют темы аренды и купли/продажи недвижимости. Сейчас читаю https://alfapromnn.ru
cost of advair
provigil otc
dexamethasone 10
how to get accutane
Не знаете, где срочно взять деньги? На канале срочные займы вы найдете самые выгодные предложения по займам на карту. Оформляйте заявки без проверок и получите деньги мгновенно. Подписывайтесь и не упустите свой шанс!
advair canada cost
Откройте двери в мир недвижимости с нашим порталом!
Получайте экспертные статьи от специалистов в области недвижимости. Узнавайте о налогах на недвижимость, осуществляйте успешные сделки купли-продажи квартир, и всегда оставайтесь в курсе последних тенденций рынка.
http://ufficioporta.ru
buy tadacip in usa
advair diskus for sale
retin a online singapore
buy cheap sildalis
buy azithromycin online
retin a 025
ventolin pill
Приветствую. Может кто знает, где найти полезные блоги о недвижимости? Хочу больше узнать про темы аренды и купли/продажи недвижимости. Пока нашла https://profmaster-vrn.ru
accutane 40 mg online
Хотите увидеть на весах минус 10 кг через 10 дней? Присоединяйтесь к каналу Похудей быстро и легко: 10 кг за 10 дней ! Мы предлагаем проверенные диеты, интенсивные тренировки и мотивационные советы. Поддержка от профессионалов поможет вам достигнуть желаемого результата. Начните сегодня!
Хотите быть в курсе всех актуальных тем в сфере недвижимости?
На нашем ресурсе вы сможете найти множество интересных статей о квартирах от застройщика, налогах на недвижимость, а также о ипотечном кредитовании.
http://zoltor24sochi.ru
老若男女のポルノ .TSfXtl6biiv
ਕਾਰਟੂਨ ਪੋਰਨੋਗ੍ਰਾਫੀ .ZdzisF8ldgJ
ਅਸੀਂ ਅਸ਼ਲੀਲ ਹਾਂ .hG6K6P53ZZv
ਪਰਿਪੱਕ (40 ) ਪੋਰਨ .5QijOmlQ4X3
Канал Кредиты на карту онлайн – ваш надежный источник информации о лучших кредитных предложениях! Мы собрали самые актуальные и выгодные варианты онлайн кредитов, а также предоставляем советы экспертов по оформлению и выбору кредита. Узнайте все о кредитной истории и будьте уверены в своих финансовых решениях.
ਕਾਰਟੂਨ ਪੋਰਨੋਗ੍ਰਾਫੀ .TeHIwY2NnZM
Wow that was odd. I just wrote an very long comment but after I clicked submit my comment didn’t show up. Grrrr… well I’m not writing all that over again. Anyways, just wanted to say great blog!
三人組ポルノ .6mrSMn0r05o
augmentin 625mg tablets
retin a 04 coupon
buy cheap nolvadex online
Приветствую. Подскажите, где почитатьразные статьи о недвижимости? Интересуют темы аренды и купли/продажи недвижимости. Сейчас читаю https://iter21.ru
buy diflucan 150 mg
ਤਿੱਕੜੀ ਪੋਰਨ .qZu1KuzLLO3
Hey there, I think your website might be having browser compatibility issues.
When I look at your website in Opera, it looks fine but when opening in Internet Explorer, it has some overlapping.
I just wanted to give you a quick heads up!
Other then that, fantastic blog!
diflucan generic coupon
baclofen 10mg tablets
An outstanding share! I’ve just forwarded this onto a friend who
had been conducting a little homework on this. And he in fact ordered me breakfast simply because I found it for him…
lol. So let me reword this…. Thank YOU for the meal!! But yeah, thanx
for spending the time to discuss this topic here on your blog.
I take pleasure in, cause I found exactly what I was taking a look for.
You’ve ended my four day lengthy hunt! God Bless you man. Have a
nice day. Bye
Заходите на наш ресурс, где вы найдете множество полезных статей на тему приемки квартиры в новостройке или покупки квартиры без отделки. Узнайте, как защитить себя от недобросовестных застройщиков, какие проверки осуществить перед покупкой жилья, и о многом другом!
http://citadel-ca.ru
Канал Потребительские кредиты – вся информация – это ваш гид в мире кредитов. Мы собрали банки, где каждый получит кредит на любые цели. Наши эксперты дают консультации и отвечают на вопросы. Узнайте о новых кредитных продуктах каждый день!
baclofen generic brand
advair 250 mcg
generic retin-a micro
Everything is very open with a really clear explanation of the
challenges. It was truly informative. Your site is very helpful.
Thanks for sharing!
advair 250 500 mg
how to get ventolin
acyclovir gel
Hello, Neat post. There’s a problem along with your website in web explorer,
could test this? IE nonetheless is the marketplace chief and a large section of folks will miss
your great writing due to this problem.
buy generic cipro
Heya i am for the first time here. I found this board and
I find It truly useful & it helped me out a lot. I’m hoping to
give something again and help others like you helped me.
For the reason that the admin of this site is working, no uncertainty very quickly it will be renowned, due to its quality contents.
I truly appreciate your technique of writing a blog. I added it to my bookmark site list and will
эффективно,
Лучшие стоматологи города, для поддержания здоровья рта,
Профессиональное лечение и консультации, для вашего уверенного выбора,
Комфортные условия и дружественный персонал, для вашей радости и улыбки,
Инновационные методы стоматологии, для вашего долгосрочного удовлетворения,
Экстренная помощь в любое время суток, для вашего здоровья и уверенности в себе,
Современное лечение заболеваний полости рта, для вашего здоровья и благополучия
лікування зубів дітям https://stomatologichnaklinikafghy.ivano-frankivsk.ua/ .
эффективно,
Лучшие стоматологи города, для вашего уверенного улыбки,
Специализированная помощь по доступным ценам, для вашей улыбки,
Бесплатная консультация и диагностика, для вашего комфорта и уверенности,
Комплексное восстановление утраченных зубов, для вашего долгосрочного удовлетворения,
Профессиональная гигиена полости рта, для вашего комфорта и удовлетворения,
Индивидуальный план лечения для каждого пациента, для вашего комфорта и удовлетворения
клініка стоматологічна https://stomatologichnaklinikafghy.ivano-frankivsk.ua/ .
generic strattera prices
На нашем сайте вы найдете полезные статьи на тему недвижимости, например, покупка квартиры в новостройке, оценка недвижимости, юридическое сопровождение сделки.
Узнайте все нюансы, которые помогут вам принять верное решение и осуществить успешную сделку с недвижимостью. Наши статьи помогут вам быть в курсе последних трендов и законов жилищного рынка, а также избежать недоразумений.
http://domzenit.ru
toradol 10mg price
advair diskus price in mexico
flomax 0.4mg
sildalis
diflucan online uk
where to buy metformin in singapore
accutane online
tamoxifen over the counter
Новые займы в СПБ – ваш путеводитель в мире выгодных онлайн займов. Мы собрали лучшие предложения от новых МФО, которые выдают займы без отказов. Неважно, есть ли у вас работа или плохая кредитная история, вы можете получить до 30 000 рублей. Первый займ часто под 0%, что делает его еще более привлекательным. Присоединяйтесь к нашему каналу и выбирайте самые выгодные условия.
Читайте полезные статьи на актуальные темы, связанные с покупкой жилья, например покупка квартиры в новостройке или налог на недвижимость.
Сайт: http://ooo-trotuar.ru
Hi there i am kavin, its my first time to commenting anyplace, when i read this piece of writing i thought i could also make comment due to this good post.
I am curious to find out what blog system you’re working with?
I’m having some small security issues with my latest blog and I’d
like to find something more risk-free. Do you have any solutions?
modafinil where to order
Thanks for some other informative website. Where else may I am getting that kind of information written in such an ideal means?
I’ve a project that I am just now working on, and I’ve been on the glance out for such information.
acyclovir 800 mg price india
baclofen for sale
I’ve read some excellent stuff here. Certainly value bookmarking for revisiting.
I wonder how so much effort you place to create this sort of fantastic informative website.
buy albuterol tablets australia
Новые займы в СПБ – ваш надежный источник информации о самых выгодных займах на карту онлайн. Мы собрали новейшие предложения от МФО, которые выдают займы без отказов и проверок. Неважно, есть ли у вас работа или плохая кредитная история, вы можете получить до 30 000 рублей. Первый займ под 0% – отличный способ улучшить ваш кредитный рейтинг. Подписывайтесь на наш канал и находите самые выгодные условия для получения займа.
dexamethasone 4 mg tablet buy online
dexamethasone uk
accutane canada cost
Всем привет! Подскажите, где найтиразные статьи о недвижимости? Пока нашел https://inter-garage.ru
I like what you guys are usually up too. This sort of clever work and exposure!
Keep up the wonderful works guys I’ve incorporated you guys to my
personal blogroll.
Всем привет! Может кто знает, где найтиполезные статьи о недвижимости? Пока нашел https://savvys-rus.ru
cipro 500mg online
diflucan online india
Hello! This is my first visit to your blog! We are a group of volunteers and starting a new project in a community in the same niche.
Your blog provided us useful information to work on. You have done a wonderful job!
Great post.
dexamethasone 10 mg
noroxin 300
эффективно,
Лучшие стоматологи города, для вашего уверенного улыбки,
Современные методы стоматологии, для вашего уверенного выбора,
Бесплатная консультация и диагностика, для вашего здоровья и благополучия,
Инновационные методы стоматологии, для вашего здоровья и красоты улыбки,
Профессиональная гигиена полости рта, для вашего здоровья и уверенности в себе,
Индивидуальный план лечения для каждого пациента, для вашего здоровья и благополучия
дитяча стоматологічна https://stomatologichnaklinikafghy.ivano-frankivsk.ua/ .
безопасно,
Индивидуальный подход к каждому пациенту, для поддержания здоровья рта,
Современные методы стоматологии, для вашей улыбки,
Бесплатная консультация и диагностика, для вашего комфорта и уверенности,
Комплексное восстановление утраченных зубов, для вашего долгосрочного удовлетворения,
Профессиональная гигиена полости рта, для вашего комфорта и удовлетворения,
Заботливое отношение и внимательный подход, для вашей уверенной улыбки
стоматологічна лікарня стоматологічна лікарня .
buy brand name accutane online
Приветствую. Подскажите, где почитатьразные статьи о недвижимости? Сейчас читаю https://optorgsib.ru
cheap diflucan
sildalis canada
Pretty component to content. I just stumbled upon your web site and in accession capital to say that I acquire actually loved account your weblog posts. Anyway I’ll be subscribing on your feeds and even I fulfillment you get admission to persistently quickly.
best generic accutane
metformin online uk
This is very attention-grabbing, You’re a very skilled blogger. I have joined your feed and sit up for in search of more of your wonderful post. Also, I have shared your site in my social networks!
provigil discount
Хотите быть в курсе всех важных тем в области недвижимости?
На нашем сайте вы найдете много полезных статей о квартирах от застройщика, а также о анализе рынка недвижимости.
Узнайте все, что вам необходимо для успешных сделок и принятия взвешенных решений в сфере недвижимости.
https://prestizh-stroi.ru
flomax price canada
roaccutane
На нашем сайте вы найдете всю необходимую информацию о недвижимости – от бронирования квартиры в новостройке до приобретения квартиры от застройщика.
Мы поможем вам выбрать лучшую квартиру на вторичном рынке, расскажем, как не ошибиться при выборе жилья и подскажем, как сэкономить на покупке.
Наш сайт: https://quartz-rsk.ru
ciprofloxacin in india
Can you be more specific about the content of your article? After reading it, I still have some doubts. Hope you can help me.
Всем привет! Может кто знает, где найтиполезные статьи о недвижимости? Пока нашел https://jkstolitsa.ru
I very delighted to find this internet site on bing, just what I was searching for as well saved to fav
amoxicillin 250mg price
flomax
What Is FitSpresso? FitSpresso is a dietary supplement that is made to support healthy fat-burning in the body
advair diskus cost in canada
Right here is the right web site for everyone who would like
to find out about this topic. You realize so much its almost hard to argue with you (not that I actually would want to…HaHa).
You definitely put a brand new spin on a subject that’s been written about for years.
Great stuff, just wonderful!
Хотите узнать всё о процессе оформления квартиры в новостройке?
Наш интернет-ресурс предлагает вам самые полезные статьи на тему покупки и продажи недвижимости.
Здесь вы найдете ответы на все вопросы и получите полную информацию о процессе оформления жилья.
https://krovlistroy.ru/
cheapest flomax uk
diflucan 200 mg tab
finasteride online bonus
buy advair on line
What’s up everyone, it’s my first go to see at this site, and piece of writing is truly fruitful in support of
me, keep up posting these content.
Definitely believe that that you stated. Your favorite reason appeared to be at the web
the easiest thing to take into accout of. I say to you, I certainly
get irked even as other people think about concerns that they plainly don’t know about.
You controlled to hit the nail upon the highest and
outlined out the entire thing with no need side effect , folks could take a signal.
Will probably be again to get more. Thanks
tadalafil singapore price
Кофе в капсулах системы Nespresso. Мы предлагаем широкий ассортимент кофе в капсулах, более 200 вкусов. Доставка СДЭК 1-3 дня в любой город Беларуси или России. Оплата при получении.
Кофе Nespresso
amoxicillin 750
buy furosemide 100 mg online
amoxicillin 250 mg capsule price
One such software that has been generating buzz these days is the Lottery Defeater
But wanna input on few general things, The website layout is perfect, the articles is really superb. “To the artist there is never anything ugly in nature.” by Franois Auguste Ren Rodin.
price of metformin 500 mg in india
Hi there, its fastidious piece of writing about media print, we all be familiar with media is a fantastic source of facts.
http://zastolje.mybb2.ru/viewtopic.php?f=86&t=13421
noroxin brand name
Выбирайте коляску Cybex для комфорта вашего ребенка, для вашего выбора.
Лучшие оферты на коляски Cybex, которые порадуют каждого.
5 причин выбрать именно коляску Cybex для вашего малыша, которые заставят вас влюбиться в этот бренд.
Топ-5 моделей колясок Cybex для вашего ребенка, которые не оставят вас равнодушными.
Элегантные решения для вашего ребенка – коляски Cybex, учитывая все особенности и пожелания.
Советы по выбору коляски Cybex для вашего малыша, исходя из индивидуальных потребностей и предпочтений.
Коляска Cybex: высокое качество и стильный дизайн, которые ценят комфорт и безопасность.
Топ-модели колясок Cybex на любой вкус и цвет, которые порадуют вас своим разнообразием и качеством.
Ключевые моменты, на которые стоит обратить внимание при выборе коляски Cybex, для вашего малыша.
Выбор коляски Cybex: что важно знать перед покупкой, чтобы сделать правильный выбор.
Топ-модели колясок Cybex для вашего малыша, которые не оставят вас равнодушными.
Лучшие модели колясок Cybex для вашей семьи, которые порадуют вас своим качеством и функционалом.
Идеальная коляска Cybex: комфорт и удобство для вашего малыша, которые стоит рассмотреть перед покупкой.
Топ-5 колясок Cybex для вашей семьи, если вы цените качество и комфорт.
Выбор коляски Cybex для вашего малыша: как не ошибиться, которые ценят надежность и стиль.
Топ-модели колясок Cybex для вашей семьи, перед совершением покупки.
Топ-5 лучших моделей колясок Cybex, исходя из личных предпочтений и потребностей.
Особенности выбора коляски Cybex: как сделать правильный выбор, которые не оставят вас равнодушными.
купить коляску cybex купить коляску cybex .
Идеальная коляска Cybex для вашего малыша, лучшие предложения.
Коляска Cybex: комфорт и безопасность в одном, для самых взыскательных.
5 причин выбрать именно коляску Cybex для вашего малыша, которые заставят вас влюбиться в этот бренд.
Идеальный выбор для заботливых родителей – коляски Cybex, которые не оставят вас равнодушными.
Элегантные решения для вашего ребенка – коляски Cybex, учитывая все особенности и пожелания.
Как правильно подобрать коляску Cybex для вашей семьи, исходя из индивидуальных потребностей и предпочтений.
Трендовые коляски Cybex для вашего малыша, которые ценят комфорт и безопасность.
Топ-модели колясок Cybex на любой вкус и цвет, которые порадуют вас своим разнообразием и качеством.
5 важных критериев при выборе коляски Cybex, для вашего малыша.
Выбор коляски Cybex: что важно знать перед покупкой, чтобы сделать правильный выбор.
Коляска Cybex: стиль, комфорт и безопасность, которые не оставят вас равнодушными.
Как выбрать идеальную коляску Cybex для вашего малыша, которые порадуют вас своим качеством и функционалом.
Как выбрать коляску Cybex: главные моменты, которые стоит рассмотреть перед покупкой.
Коляска Cybex для вашего малыша: лучшие модели, если вы цените качество и комфорт.
Выбор коляски Cybex для вашего малыша: как не ошибиться, которые ценят надежность и стиль.
Новинки колясок Cybex, которые стоит рассмотреть, перед совершением покупки.
Коляска Cybex: безопасность и комфорт для вашего малыша, исходя из личных предпочтений и потребностей.
Особенности выбора коляски Cybex: как сделать правильный выбор, которые не оставят вас равнодушными.
коляска cybex коляска cybex .
Hello, Neat post. There’s a problem with your web site in internet explorer, might
check this? IE nonetheless is the market leader and a huge component of other folks will leave out your excellent writing because of this problem.
furosemide 40 mg tablet
I was recommended this website by my cousin. I am not sure whether this post is written by him
as no one else know such detailed about my trouble.
You’re amazing! Thanks!
Лучшие модели колясок Tutis, Как выбрать идеальную коляску от Tutis?, секреты правильного выбора, Инструкция по эксплуатации коляски Tutis, инструкция для новичков, что приобрести для удобства, лучшие модели для спортивных прогулок, Как правильно ухаживать за коляской Tutis?, чтобы сохранить отличное состояние, правила использования коляски, секреты комфортного выезда, Почему Tutis лучше всего подходит для вашей семьи?, Почему Tutis – марка будущего, Как выбрать коляску Tutis с максимальным комфортом для ребенка?, профессиональное мнение, Почему Tutis – выбор сознательных семей, преимущества использования коляски Tutis
коляска 3 в 1 тутис коляска 3 в 1 тутис .
Самые популярные коляски Tutis, для стильных семей, секреты правильного выбора, Секреты долговечности и надежности коляски Tutis, Лучшее дополнение к вашей коляске от Tutis, аксессуары, которые сделают вашу жизнь проще, Как не ошибиться с выбором между Tutis и другими марками, Инструкция по уходу за коляской Tutis, советы по уходу, Секреты комфортной поездки с Tutis, рекомендации для родителей, Почему Tutis лучше всего подходит для вашей семьи?, секреты успешного выбора, секреты качественного производства, рекомендации экспертов, Почему Tutis – выбор сознательных семей, надежность и комфорт в каждом шаге
коляска tutis цена коляска tutis цена .
cloridrato de vardenafil
geinoutime.com
과거에는 의심이 있었지만 결국 깊이 생각하지 않았습니다.
baclofen 30 mg
vermox tablet price
can i buy vermox over the counter
Admiring the commitment you put into your blog and detailed information you provide. It’s nice to come across a blog every once in a while that isn’t the same old rehashed material. Wonderful read! I’ve saved your site and I’m including your RSS feeds to my Google account.
http://www.arusak-attestats24.com
Hi this is kind of of off topic but I was wondering if blogs use WYSIWYG editors or if you have to manually code with HTML. I’m starting a blog soon but have no coding know-how so I wanted to get advice from someone with experience. Any help would be greatly appreciated!
noroxin 400 mg tablets
Всем привет! Подскажите, где найтиполезные блоги о недвижимости? Пока нашел https://master-architector.ru
flomax over the counter
amoxicillin 250mg for sale
can you buy albuterol in mexico
price of 21 acyclovir
Good post and straight to the point. I am not sure if this is actually the best place to ask but do you people have any ideea where to employ some professional writers? Thank you 🙂
buy azithromycin 1000 mg
zovirax price nz
augmentin 500 mg price
toradol for fever
buy diflucan
buy retin a online uk
bactrim 160 800 mg tablets
What Is Puravive? Puravive is an herbal weight loss supplement that supports healthy weight loss in individuals.
Всем привет! Интересные статьи о недвижимости. Аренда, купля/продажа, недвижимость как бизнес. Подробнее http://sma-repair.ru
Читайте полезные статьи на актуальные темы, связанные с покупкой жилья, например квартира от застройщика или ликвидационная стоимость недвижимости.
Сайт: https://ooo-trotuar.ru
azithromycin 250 mg price in india
Amazing! This blog looks just like my old one! It’s on a entirely different subject but it has pretty much the same page layout and design. Superb choice of colors!
baclofen 10 mg tablets
Thank you for sharing superb informations. Your web-site is very cool. I’m impressed by the details that you¦ve on this blog. It reveals how nicely you perceive this subject. Bookmarked this website page, will come back for extra articles. You, my friend, ROCK! I found just the information I already searched everywhere and simply couldn’t come across. What an ideal web-site.
baclofen tablets
This text is priceless. When can I find out more?
Будьте в курсе всех событий в мире смешанных единоборств вместе с Octagon Express! Узнавайте самые свежие новости ММА на нашем сайте. Мы предлагаем эксклюзивные интервью с бойцами, аналитические статьи и обзоры турниров. Не пропустите ни одной важной новости и всегда оставайтесь в центре событий. Подписывайтесь на обновления и следите за всеми важными событиями в мире ММА с Octagon Express!
Hello I am so glad I found your site, I really found you by error, while I was looking on Askjeeve for something else, Anyways I am here now and would just like to say kudos for a remarkable post and a all round interesting blog (I also love the theme/design), I don’t have time to browse it all at the minute but I have bookmarked it and also included your RSS feeds, so when I have time I will be back to read a lot more, Please do keep up the fantastic job.
http://http://musey-uglich.ru/
Hello there! Would you mind if I share your blog with my myspace group? There’s a lot of folks that I think would really enjoy your content. Please let me know. Cheers
http://www.musey-uglich.ru
provigil for sale
diflucan 110 mg
Does your blog have a contact page? I’m having trouble locating it but, I’d like to shoot you an email. I’ve got some recommendations for your blog you might be interested in hearing. Either way, great blog and I look forward to seeing it improve over time.
Great article.
В нашем мире, где диплом – это начало успешной карьеры в любой сфере, многие стараются найти максимально простой путь получения качественного образования. Наличие официального документа переоценить попросту невозможно. Ведь диплом открывает двери перед каждым человеком, который желает начать профессиональную деятельность или продолжить обучение в высшем учебном заведении.
В данном контексте наша компания предлагает оперативно получить этот важный документ. Вы сможете заказать диплом старого или нового образца, и это становится удачным решением для человека, который не смог закончить образование, утратил документ или хочет исправить свои оценки. Любой диплом изготавливается аккуратно, с максимальным вниманием ко всем элементам, чтобы в итоге получился полностью оригинальный документ.
Плюсы такого подхода заключаются не только в том, что вы максимально быстро получите свой диплом. Процесс организовывается удобно, с профессиональной поддержкой. От выбора требуемого образца до консультации по заполнению личных данных и доставки в любое место страны — все находится под полным контролем качественных мастеров.
Всем, кто пытается найти быстрый способ получения необходимого документа, наша компания предлагает выгодное решение. Купить диплом – значит избежать долгого процесса обучения и сразу перейти к достижению собственных целей, будь то поступление в ВУЗ или начало удачной карьеры.
http://http://seoyour.ru/
baclofen 50 mg
Интересуетесь последними результатами боев UFC? На Octagon Express вы найдете самые свежие и детальные результаты боев UFC. Узнайте, кто вышел победителем, и читайте аналитические отчеты о каждом поединке. Будьте всегда в курсе всех событий и не пропустите ни одной важной детали. Подписывайтесь на обновления и следите за всеми результатами вместе с Octagon Express!
where to buy azithromycin 250 mg
гейтс оф олимпус на деньги гейтс оф олимпус на деньги .
Хотите узнать, когда и где будут проходить самые захватывающие бои UFC? Посетите Octagon Express для получения актуального расписания боев UFC. Следите за датами и временем предстоящих поединков, чтобы не пропустить ни одного важного события. Подписывайтесь на обновления и оставайтесь в курсе всех турниров и боев с Octagon Express. Погрузитесь в мир UFC и наслаждайтесь каждым поединком!
advair 125
buy cipro online
cipro canada
Хотите узнать самые горячие новости из мира бокса? Octagon Express представляет вам главные новости бокса на сегодня! Свежие интервью, захватывающие видео и аналитические обзоры – все это ждет вас на нашем сайте. Следите за всеми важными событиями и не пропустите ни одной сенсации. Подписывайтесь на обновления и будьте первым, кто узнает все последние новости из мира бокса вместе с Octagon Express!
geinoutime.com
이것은 가족의 기둥이며 열에 아홉은 유일한 것입니다.
lasix 100 mg online
В современном мире, где диплом – это начало удачной карьеры в любой сфере, многие ищут максимально простой путь получения качественного образования. Наличие официального документа сложно переоценить. Ведь именно он открывает дверь перед каждым человеком, желающим начать профессиональную деятельность или продолжить обучение в высшем учебном заведении.
Мы предлагаем максимально быстро получить этот необходимый документ. Вы можете приобрести диплом, что является отличным решением для всех, кто не смог закончить обучение, потерял документ или желает исправить плохие оценки. диплом изготавливается аккуратно, с максимальным вниманием ко всем элементам, чтобы на выходе получился документ, 100% соответствующий оригиналу.
Преимущество такого решения состоит не только в том, что вы быстро получите свой диплом. Весь процесс организован удобно и легко, с профессиональной поддержкой. Начиная от выбора необходимого образца до правильного заполнения личных данных и доставки по России — все под абсолютным контролем наших мастеров.
Для всех, кто хочет найти оперативный способ получить требуемый документ, наша компания предлагает отличное решение. Заказать диплом – это значит избежать долгого обучения и сразу перейти к своим целям, будь то поступление в университет или начало успешной карьеры.
http://seoyour.ru/
flomax inhaler
provigil generic
свит бонанза на деньги свит бонанза на деньги .
Your article helped me a lot, is there any more related content? Thanks!
baclofen cheapest
cipro 750 mg tablet
cost of metformin in canada
tamoxifen 20 mg tablet
What is Renew? Renew is a dietary supplement designed to support blood flow while also aiming to boost testosterone levels andprovide an explosive energy drive
I just couldn’t depart your site prior to suggesting that I really enjoyed the standard info a person provide for your visitors? Is gonna be back often to check up on new posts
purchase nolvadex
advair diskus 500 mcg
amoxicillin price uk
As a Newbie, I am constantly searching online for articles that can benefit me. Thank you
lasix diuretic
buy generic advair from canada
furosemide order online
amoxil capsule price
пожаловаться на сайт мошенников пожаловаться на сайт мошенников .
Приобрести устройство скважины на воду можно на сайте мастер-буров.рф прямо сейчас. Скважина с чистой водой — один из важных компонентов на Вашем участке. Мы гарантируем качество работы, материалов, а также осуществляем сервисное обслуживание. Внешние факторы могут негативно влиять на скважину и качество воды, мы также работаем с восстановлением поврежденных скважин от разрушения и с очисткой от заиливания. Звоните, приходите, будем рады с Вами работать.
diflucan
крейзи манки играть онлайн crazy-monkey-ru.ru .
Откройте для себя удивительный мир турецких сериалов на сайте turkvideo.tv. Здесь вы сможете смотреть турецкие сериалы на русском языке, наслаждаясь великолепной озвучкой и высоким качеством. Каждая история, каждая серия захватывает дух и увлекает в незабываемое путешествие. Насладитесь драмами, романтическими историями и приключениями без ограничений. Присоединяйтесь к нашим зрителям и откройте для себя новые эмоции и впечатления от просмотра лучших турецких сериалов на русском языке.
geinoutime.com
지난 며칠 동안 Xiao Eunuch는 잘 알려진 성질이 나빴습니다.
Откройте для себя мир турецких сериалов на русском языке на сайте turkvideo.tv. Здесь вы найдете широкий выбор захватывающих сюжетов и популярных актеров, доступных для просмотра в отличном качестве. Посетите раздел турецкие сериалы на русском языке, чтобы наслаждаться любимыми сериалами без необходимости искать переводы. Этот сайт идеально подходит для всех любителей турецкого кинематографа, предлагая удобный доступ к лучшим сериалам Турции с русской озвучкой. Присоединяйтесь и начните смотреть уже сегодня!
Относительно скважины иркутск цена мы вам непременно поможем. На данном онлайн портале можно увидеть приблизительную глубину бурения на собственном участке в видео, а также цены. Но самый безошибочный способ — это позвать к себе мастера для выявления верного места под скважину, определения объема работы и, в соответствии с этим, стоимость. Напишите контактный номер и мы свяжемся с Вами в скорое время.
Откройте для себя мир магии и приключений на сайте turkvideo.tv, где вы можете смотреть турецкие сериалы фэнтези. Мы гордимся тем, что занимаем первое место в Google и Yandex, предлагая сериалы в высоком HD качестве без назойливой рекламы. Наслаждайтесь увлекательными историями, полными волшебства и мифических существ. Каждый сериал перенесет вас в фантастические миры, где возможны самые невероятные приключения. Начните свое путешествие в мир турецкого фэнтези на turkvideo.tv уже сегодня!
I’m not that much of a online reader to be honest but your sites really nice, keep it up!
I’ll go ahead and bookmark your site to come back down the road.
All the best
Приветствую. Может кто знает, где найтиполезные статьи о недвижимости? Сейчас читаю https://ak-3.ru
Fantastic goods from you, man. I’ve understand your stuff
previous to and you’re just too wonderful. I really like what
you’ve acquired here, really like what you’re stating and the way in which you say it.
You make it entertaining and you still take care of to keep it wise.
I cant wait to read much more from you. This is actually a wonderful website.
What i don’t understood is in truth how you are not really a lot more well-appreciated than you
may be right now. You are very intelligent. You recognize therefore
considerably in the case of this matter, produced me individually consider it
from a lot of various angles. Its like men and women are not involved until it
is one thing to accomplish with Girl gaga! Your personal stuffs outstanding.
At all times take care of it up!
Приветствую. Подскажите, где почитатьполезные блоги о недвижимости? Пока нашел https://417-017.ru
advair diskus 500 mcg 50 mcg
Секрет популярности теневого плинтуса
теневой плинтус стоимость теневой плинтус стоимость .
Идеальное решение для уютного дома – плинтус теневой.
теневой плинтус скрытого монтажа теневой плинтус скрытого монтажа .
generic cipro
аккаунт телеграмм купить аккаунт телеграмм купить .
Приветствую. Подскажите, где почитатьполезные статьи о недвижимости? Пока нашел https://aquatopnn.ru
Всем привет! Подскажите, где почитатьполезные статьи о недвижимости? Пока нашел https://artem-dvery.ru
metformin online canada drug
Бесплатный хостинг в Беларуси: качество и надежность, плюсы и минусы.
Сравниваем лучшие предложения хостинга в Беларуси, инструкции и рекомендации.
RAIDHOST, HOSTERO, TUT.BY: лучшие бесплатные хостинги в Беларуси, оценка и обзор.
Как перенести сайт на бесплатный хостинг в Беларуси?, шаги и рекомендации.
Безопасность сайта: SSL на хостинге в Беларуси бесплатно, за и против.
Простая инструкция: создание сайта на бесплатном хостинге в Беларуси, шаги и советы.
Где можно купить хостинг в Беларуси дешево и качественно?, прогноз и анализ.
Виртуальный хостинг бесплатно https://gerber-host.ru/ .
Хостинг в Беларуси бесплатно: лучший выбор для вашего сайта, преимущества и особенности.
Бесплатные хостинги в Беларуси: что выбрать?, советы и рекомендации.
3 лучших хостинга в Беларуси бесплатно: наши рекомендации, оценка и обзор.
Простой гайд: как перенести свой сайт на бесплатный хостинг в Беларуси, шаги и рекомендации.
SSL-сертификаты на бесплатных хостингах в Беларуси: важный момент, характеристики и обзор.
Как создать сайт на бесплатном хостинге в Беларуси?, инструкция и рекомендации.
Где можно купить хостинг в Беларуси дешево и качественно?, характеристики и отзывы.
Рейтинг хостингов Беларуси https://gerber-host.ru/ .
generic accutane for sale
Приветствую. Может кто знает, где найтиполезные статьи о недвижимости? Пока нашел https://asiatreid.ru
Всем привет! Может кто знает, где найтиполезные статьи о недвижимости? Пока нашел https://dilerskiy-tsentr-baumit.ru
Всем привет! Подскажите, где почитатьполезные блоги о недвижимости? Пока нашел https://dompodkluch33.ru
Всем привет! Подскажите, где почитатьразные блоги о недвижимости? Пока нашел https://eniseyburvod.ru
For most up-to-date news you have to pay a quick visit world wide web and on the web I found this website as a most excellent web site for hottest updates.
forum.drustvogil-galad.si/index.php?topic=10004.0
mydoggymatch.com/read-blog/601_where-to-order-a-diploma-or-certificate-at-a-adequate-price.html?mode=night
alter-energo.ru/topic2861.html?view=previous
levit.in.ua/about-us.html
http://www.85sucai.com/member/index.php?uid=yhicyp
Всем привет! Подскажите, где почитатьразные блоги о недвижимости? Пока нашел https://etalon-voda.ru
cost cipro
I’m not sure why but this web site is loading extremely slow for me. Is anyone else having this problem or is it a issue on my end? I’ll check back later on and see if the problem still exists.
zainexxtechno.com/slot-poseidons-rising
hoisuhoc.vn/tong-hop-nhung-mon-an-giup-thai-nhi-tang-can-tot-nhat/
cn-agent.com/c_feedback/index.asp?page=10
ks-elektronika.pl/product_ask_avaliable.php?products_id=71
tnrevergreen.com.vn/dien-tich-tim-tuong-la-gi-mua-nha-nen-dung-cach-tinh-dien-tich-nao/
Всем привет! Может кто знает, где найтиразные блоги о недвижимости? Пока нашел https://floor-ashton.ru
Приветствую. Подскажите, где почитатьразные блоги о недвижимости? Сейчас читаю https://gismt72.ru
Приветствую. Подскажите, где почитатьразные блоги о недвижимости? Сейчас читаю https://kait-volga.ru
Приветствую. Может кто знает, где почитатьполезные блоги о недвижимости? Пока нашел https://kaluga-elite.ru
Приветствую. Может кто знает, где почитатьполезные статьи о недвижимости? Пока нашел https://kamenolomnya43.ru
Can you tell us more about this? I’d care to find out more details.
Great beat ! I wish to apprentice while you amend your web site, how could i subscribe for a
blog site? The account aided me a acceptable deal. I had
been tiny bit acquainted of this your broadcast offered
bright clear concept
에그벳
Fang 가족의 규모는 Huangjinzhou에서 매우 크며 지난 몇 년 동안 더욱 끔찍해졌습니다.
Приветствую. Может кто знает, где почитатьразные блоги о недвижимости? Пока нашел https://kmzperm.ru
Hello I am so grateful I found your weblog, I really found you by accident, while I was researching on Aol for something else, Anyhow I am here now and would just like to say thank you for a marvelous post and a all round exciting blog (I also love the theme/design), I don’t have time to go through it all at the minute but I have bookmarked it and also added your RSS feeds, so when I have time I will be back to read a great deal more, Please do keep up the fantastic jo.
worldavtonew.ru/page/3
we-are-family.ru/contact.htm
mipon.net/bbs-c/clever.cgi/clever.cgi?page=280
img-group.ru/Partners.html
forum.l2star.net/member.php?u=17186
Приветствую. Подскажите, где почитатьполезные статьи о недвижимости? Сейчас читаю https://kovry159.ru
Топ-5 книг о pin up культуре, которые нужно прочитать
pin up oficial https://pinupbrazilnbfdrf.com/ .
Всем привет! Подскажите, где почитатьполезные блоги о недвижимости? Пока нашел https://krepegmaster.ru
жиросжигатель http://www.www.ozon.ru/product/nexis-effektivnye-tabletki-dlya-pohudeniya-zhiroszhigatel-dlya-zhenshchin-60-kapsul-kurs-na-mesyats-1564574748/ .
Всем привет! Подскажите, где найтиполезные блоги о недвижимости? Сейчас читаю https://kuler-tsentr.ru
Всем привет! Подскажите, где найтиполезные блоги о недвижимости? Сейчас читаю https://liem-com.ru
Всем привет! Подскажите, где почитатьполезные статьи о недвижимости? Пока нашел https://oscltd.ru
Hi just wanted to give you a brief heads up and let you know a few of the images aren’t loading properly. I’m not sure why but I think its a linking issue. I’ve tried it in two different internet browsers and both show the same outcome.
http://www.sskyn.com/home-uid-82653.html
microstockhowto.com/tag/community/
crosspromote.click/index.php?do=/public/user/blogs/name_Alanpoe/page_7/
1-carat.ru/
tirserwis-lublin.pl/mapka.html
Всем привет! Может кто знает, где почитатьполезные статьи о недвижимости? Сейчас читаю https://ppu-odk.ru
Завод из России продает разборные гантели на https://Razbornye-ganteli.ru по низким ценам. Для тренировок в квартире – это самый лучший комплект с маленькими размерами и большой функциональностью. Продаются в полном наборе с замками и грифами для гантелей.Отягощения сборные дают возможность заниматься с любой массой. Предлагаем разнообразный выбор продуктов от ведущих брендов в сетевом магазине.
Лучший выбор военной экипировки|Ваш надежный партнер в выборе военных товаров|Здесь найдете все для военного дела|Армейские товары по выгодным ценам|Выбор настоящих военных победителей|Защита и безопасность в вашем распоряжении|Боевая техника для суровых реалий|Армейский магазин с широким ассортиментом|Выбирайте только профессиональное снаряжение|Снаряжение от лучших производителей|Качественная экипировка для армии|Боевая техника для самых сложных задач|Только качественные товары для военного применения|Купите только проверенные военные товары|Амуниция и снаряжение от лучших производителей|Экипировка для защитников Отечества|Армейский магазин с широким выбором экипировки|Купите профессиональное снаряжение для службы|Выбор настоящих защитников|Выбирайте только надежные военные товары
магазин військового одягу https://magazinvoentorg.kiev.ua/ .
Широчайший ассортимент военных товаров|Оружие и снаряжение для настоящих мужчин|Здесь найдете все для военного дела|Армейские товары по выгодным ценам|Оружие и аксессуары для профессионалов|Защита и безопасность в вашем распоряжении|Военная экипировка от лучших брендов|Армейский магазин с широким ассортиментом|Выбирайте только профессиональное снаряжение|Снаряжение от лучших производителей|Снаряжение для профессионалов военного дела|Боевая техника для самых сложных задач|Только качественные товары для военного применения|Купите только проверенные военные товары|Выбор профессионалов в военной сфере|Экипировка для защитников Отечества|Армейский магазин с широким выбором экипировки|Специализированный магазин для военных сотрудников|Выбор настоящих защитников|Выбирайте только надежные военные товары
магазин військовий https://magazinvoentorg.kiev.ua/ .
dexona tablet price
Приветствую. Может кто знает, где почитатьразные блоги о недвижимости? Сейчас читаю https://redglade-nn.ru
baclofen 50 mg
Приветствую. Подскажите, где найтиполезные статьи о недвижимости? Пока нашел https://santam1.ru
Приветствую. Может кто знает, где найтиполезные статьи о недвижимости? Пока нашел https://sibarit54.ru
I enjoy your piece of work, thankyou for all the useful articles.
купить диплом в череповце diplomvash.ru .
Приветствую. Может кто знает, где найтиразные блоги о недвижимости? Сейчас читаю https://stroyproektm.ru
Всем, кто ищет турецкие сериалы бесплатно, рекомендую сайт turkline.tv. Огромный выбор сериалов различных жанров, все в HD 1080 и с русской озвучкой. Сайт не содержит рекламы, что делает просмотр еще более приятным. Все сериалы доступны абсолютно бесплатно, что особенно радует. Турклайн.тв – лучший выбор для бесплатного просмотра турецких сериалов онлайн.
dexamethasone 2mg tablets price
Hi there, after reading this awesome article i am as well glad to share my experience here with mates.
longlive.com/node/1080
horordark.ru/page/8
cogita.site/news/otchety/andrei-scherbak.-gosudarstvo-i-malyi-biznes-ruka-dayuschaya-i-ruka-karayuschaya
mrkarpiuk.xaa.pl/boards/shopping/showthread.php?tid=37149&pid=128995
topextern.ru/zhizn-biznesa-v-2020-godu.html
Всем привет! Может кто знает, где почитатьразные блоги о недвижимости? Сейчас читаю https://tent44.ru
Всем привет! Подскажите, где почитатьразные статьи о недвижимости? Сейчас читаю https://universal37.ru
buy strattera canada
Приветствую. Может кто знает, где найтиразные блоги о недвижимости? Пока нашел https://velikaya-stena.ru
купить диплом в архангельске купить диплом в архангельске .
Искал платформу, где можно турецкий сериал смотреть онлайн на русском, и нашел turkline.tv. Сайт радует большим выбором сериалов и удобным интерфейсом. Качество перевода на русском языке позволяет полностью погрузиться в сюжет. Каждый вечер я наслаждаюсь просмотром нового сериала, и turkline.tv всегда под рукой. Рекомендую этот сайт всем любителям турецкого кино.
Всем привет! Подскажите, где найтиразные блоги о недвижимости? Пока нашел https://zmk-54.ru
Good post. I learn something new and challenging on sites I stumbleupon everyday. It’s always interesting to read content from other writers and use something from their sites.
serialforfree.ru/page/7
regullife.ru/index.php?links_exchange=yes&show_all=yes&page=40
sadovod63.ru/products
e-maxx.ru/forum/profile.php?id=19116
http://www.miranetwork.it/index.php?option=com_k2&view=itemlist&task=user&id=434690
aviator game website http://www.aviator-games-online.ru/ .
Hi are using WordPress for your blog platform? I’m new to the blog world but I’m trying to get started and set up my own. Do you need any coding knowledge to make your own blog? Any help would be greatly appreciated!
artem-energo.ru/forums.php?m=posts&q=17775
xianz.com/index.php?mode=messages&act=compose&rec_id=47561
http://www.ba98.org/contact.php?sujet=6
allukrnews.ru/put-k-professionalnomu-priznaniyu-pokupka-diploma-kak-reshenie/
opengadjet.ru/page/4
Искал новинки турецких сериалов и наткнулся на смотреть турецкие сериалы 2023 онлайн на turkline.tv. Меня приятно удивило, что все сериалы доступны в HD качестве и совершенно бесплатно. Навигация по сайту очень удобная, а отсутствие рекламы делает просмотр комфортным. Порадовал большой выбор жанров – от драм до комедий. Очень рад, что нашел этот сайт и рекомендую его всем любителям турецких сериалов. Турклайн.тв – лучший выбор для просмотра новых сериалов 2023 года.
zovirax 5
игра лаки джет на деньги https://www.1win-luckyjet-game.ru .
I am curious to find out what blog system you are working with?
I’m experiencing some minor security issues with my latest website and I would like
to find something more safeguarded. Do you have any
recommendations?
Охрана труда онлайн обучение safetysystemsgroup.com
Помимо проведение оценки профессиональных рисков по охране труда у нас Вы найдете курсы по обучению в режиме онлайн по охране труда, пожарно-технический минимум, электробезопасность 4-я группа и другие. Свяжитесь с нами по вышеуказанному телефону, адресу или закажите возвратный звонок. Будем рады сотрудничеству.
Awesome issues here. I’m very glad to see your post. Thanks a lot and I am taking a look ahead to contact you. Will you kindly drop me a mail?
zebuskape.com/estate-planning-1
clickandconnectclubs.com/index.php?do=/public/blog/view/id_119636/title_-2024/
http://www.bakili-fclub.com/elaqeen.html
opengadjet.ru/page/4
finttech.ru/page/36
Your house is valueble for me. Thanks!…
Группы обучения по охране труда safetysystemsgroup.com
Кроме заказать оценку профессиональных рисков по охране труда у нас Вы найдете курсы по обучению в режиме онлайн по охране труда, пожарно-технический минимум, электробезопасность 4-я группа и другие. Свяжитесь с нами по вышеупомянутому номеру телефона, адресу или закажите обратный звонок. Мы будем рады работать с Вами.
What’s up, I want to subscribe for this website to take most up-to-date updates, therefore where can i do it please help out.
ultras.lv/topic1669.html?view=print
allonlinesport.ru/page/14/
share-design.ru/legal-notice/
truyen.biz/doi-anh-em-ba-dao-chapter-22/
virusinfo.info/cpstyles/vB/?gde_kupit_diplom_o_srednem_obrazovanii.html
Thank you for the good writeup. It in truth used to be a entertainment account it. Glance complicated to far brought agreeable from you! By the way, how can we keep in touch?
newspromworld.ru/page/2
forumaniga.me/member/414-uf_23829059/visitormessage/13030-%D0%BF%D1%83%D0%B1%D0%BB%D0%B8%D1%87%D0%BD%D0%BE%D0%B5-%D1%81%D0%BE%D0%BE%D0%B1%D1%89%D0%B5%D0%BD%D0%B8%D0%B5-%D0%BE%D1%82-uf_23829059
ruyanamerica.com/News/News.cfm?NewsID=1003
http://www.djwx.com/forums/user/profile/64386.page
krutovo.ru/index.php?name=Account&op=info&uname=ymonozav
Когда я искал турецкие сериалы 2024 онлайн, наткнулся на turklife.tv. Сайт поразил меня разнообразием жанров и удобным разделением сериалов по годам. Все новинки 2024 года здесь доступны бесплатно, без регистрации и рекламы, и в отличном HD качестве с русской озвучкой.
Люблю смотреть турецкие сериалы за их увлекательные сюжеты и харизматичных героев. Теперь я всегда в курсе новинок благодаря turklife.tv – это лучшее место для просмотра любимых сериалов!
Классная тема! Кстати, вот классная статья о подключении Яндекс Плюс: https://taplink.cc/kak_podkliuchit_iandeks_plius Может, кому пригодится..
I absolutely love your blog and find many of your post’s to be exactly I’m looking for. Do you offer guest writers to write content for you personally? I wouldn’t mind publishing a post or elaborating on a lot of the subjects you write related to here. Again, awesome site!
yenko.net/forum/member.php?tab=visitor_messaging&u=70162
avtoweek2016.ru/page/4/
newfinbiz.ru/page/13
http://www.taijiacademy.com/newforum_down/profile.php?mode=viewprofile&u=300836
we-are-family.ru/contact.htm
открытие замков цена открытие замков цена .
Приветствую. Подскажите, где почитатьразные блоги о недвижимости? Сейчас читаю https://417-017.ru
Хотите погрузиться в мир эмоций и захватывающих историй? Заходите на turklife.tv и смотрите турецкие сериалы драмы! Здесь вас ждут лучшие драматические сериалы в HD 1080 качестве и с профессиональной русской озвучкой. Турклайф ТВ предлагает широкий выбор драм на любой вкус, от новинок 2024 года до классических хитов.
Каждый день добавляются новые серии, и всё это абсолютно бесплатно и без рекламы. Откройте для себя мир турецких драм на turklife.tv – здесь вы найдете всё, что искали!
Меня пригласили на свадьбу лучшей подруги, но денег на подарок и наряд не было. К тому же, у меня были просрочки по другим кредитам. Я начала искать решение в интернете и нашла в Яндексе на первом месте Телеграм канал мфо малоизвестные без отказа . Это сразу вызвало доверие. На канале я нашла много новых МФО, которые давали займы всем. Оформила займ всего за 10 минут, и деньги быстро поступили на мой счет. Смогла купить красивый наряд и хороший подарок. Всем советую подписаться на этот канал!
Всем привет! Подскажите, где найтиразные блоги о недвижимости? Сейчас читаю https://aquatopnn.ru
Недавно друзья посоветовали мне сайт turklife.tv, и это оказалось настоящей находкой! Здесь можно турецкие сериалы 2024 на русском языке смотреть в отличном HD качестве с идеальной озвучкой. Сайт предлагает огромное количество жанров и все сериалы удобно разбиты по годам.
Что особенно приятно, так это отсутствие регистрации и рекламы. Я обожаю турецкие сериалы за их захватывающие сюжеты и ярких персонажей, и теперь у меня есть идеальное место для их просмотра – turklife.tv!
You’ve made some really good points there.
I looked on the net to find out more about the issue and found most
individuals will go along with your views on this site.
Всем привет! Подскажите, где найтиразные статьи о недвижимости? Сейчас читаю https://artem-dvery.ru
Шаги к получению лицензии на недвижимость|Все, что вам нужно знать о лицензии на недвижимость|Станьте лицензированным агентом по недвижимости|Секреты быстрого получения лицензии на недвижимость|Разберитесь в процессе получения лицензии на недвижимость|Следуйте этим шагам для получения лицензии на недвижимость|Простой путь к получению лицензии на недвижимость|Изучите основы получения лицензии на недвижимость|Эффективные стратегии получения лицензии на недвижимость|Лицензия на недвижимость для начинающих: советы и рекомендации|Процесс получения лицензии на недвижимость: как это работает|Секреты скорого получения лицензии на недвижимость|Легкий путь к получению лицензии на недвижимость|Топ советы по получению лицензии на недвижимость|Профессиональные советы по получению лицензии на недвижимость|Разберитесь в процессе получения лицензии на недвижимость: полное руководство|Получение лицензии на недвижимость: лучшие практики и советы|Как быстро и легко получить лицензию на недвижимость|Ключевые моменты получения лицензии на недвижимость|Легко получите лицензию на недвижимость с этими советами|Как стать агентом по недвижимости с лицензией|Как получить лицензию на недвижимость быстро и легко|Инструкция по получению лицензии на недвижимость|Секреты быстрого получения лицензии на недвижимость|Эффективные советы по успешному получению лицензии на недвижимость|Сек
Alabama Real Estate Licence https://realestatelicensehefrsgl.com/states/alabama-real-estate-license/ .
Как получить лицензию на недвижимость|Все, что вам нужно знать о лицензии на недвижимость|Подробное руководство по получению лицензии на недвижимость|Секреты быстрого получения лицензии на недвижимость|Инструкция по получению лицензии на недвижимость|Полезные советы по получению лицензии на недвижимость|Лицензия на недвижимость: важные аспекты|Шаг за шагом к лицензии на недвижимость|Эффективные стратегии получения лицензии на недвижимость|Успешное получение лицензии на недвижимость: шаг за шагом|Основные моменты получения лицензии на недвижимость|Полезные советы по получению лицензии на недвижимость|Легкий путь к получению лицензии на недвижимость|Как стать агентом по недвижимости с лицензией: пошаговое руководство|Советы по получению лицензии на недвижимость от профессионалов|Эффективные стратегии для успешного получения лицензии на недвижимость|Шаги к успешной лицензии на недвижимость|Как быстро и легко получить лицензию на недвижимость|Лицензия на недвижимость: ключ к успеху в индустрии недвижимости|Три шага к успешной лицензии на недвижимость|Получите лицензию на недвижимость и станьте профессиональным агентом|Как получить лицензию на недвижимость быстро и легко|Инструкция по получению лицензии на недвижимость|Секреты быстрого получения лицензии на недвижимость|Как получить лицензию на недвижимость: основные принципы и стратегии|Сек
How to get a real estate license in California How to get a real estate license in California .
잘 터지는 슬롯
“곡물, 기름, 포도주, 모든 것을 높은 가격으로 받으십시오!”
슬롯 무료
그런데 아버지의 유골을 어떻게 찾았는지 정말 모르십니까?
Приветствую. Может кто знает, где почитатьразные блоги о недвижимости? Сейчас читаю https://asiatreid.ru
создание и продвижение сайтов в москве цена https://prodvizhenie-sajtov-v-moskve117.ru/ .
Приветствую. Подскажите, где найтиполезные блоги о недвижимости? Сейчас читаю https://dilerskiy-tsentr-baumit.ru
hello!,I like your writing very much! share we communicate more about your article on AOL? I require an expert on this area to solve my problem. May be that’s you! Looking forward to see you.
Заходите на наш сайт, где вы найдете большое количество полезных статей на тему приемки квартиры в новостройке или покупки квартиры без отделки. Узнайте, как защитить себя от недобросовестных застройщиков, какие проверки осуществить перед покупкой жилья, и о многом другом!
https://citadel-ca.ru
Приветствую. Может кто знает, где почитатьразные блоги о недвижимости? Пока нашел https://dompodkluch33.ru
На нашем сайте вы найдете информационные статьи на тему недвижимости, например, отделка квартиры с нуля, продажа и покупка недвижимости, юридическое сопровождение сделки.
Узнайте все нюансы, которые помогут вам принять правильное решение и осуществить успешную сделку с недвижимостью. Наши статьи помогут вам быть в курсе последних трендов и законов жилищного рынка, а также избежать ошибок.
http://domzenit.ru
Приветствую. Подскажите, где найтиполезные статьи о недвижимости? Пока нашел https://eniseyburvod.ru
Читайте полезные статьи на важные темы, связанные с продажей жилья, например приемка квартиры в новостройке или стоимость недвижимости в Москве.
Сайт: https://ooo-trotuar.ru
Приветствую. Подскажите, где найтиполезные статьи о недвижимости? Сейчас читаю https://etalon-voda.ru
Приветствую. Подскажите, где найтиполезные статьи о недвижимости? Сейчас читаю https://floor-ashton.ru
Почему стоит построить дом из бруса 9х12 | Подбор проекта для дома из бруса 9х12 | Секреты уютного интерьера в доме из бруса 9х12 | Как создать уютный интерьер в доме из бруса 9х12 | Выбор фундамента для дома из бруса 9х12 | Выбор фундамента для дома из бруса 9х12 | Современные технологии строительства дома из бруса 9х12 | Топ-5 мебельных трендов для дома из бруса 9х12 | Для комфортного отдыха: зона lounge в доме из бруса 9х12 | Как рассчитать бюджет на строительство дома из бруса 9х12
дома из бруса 9х12 https://domizbrusa-9x12spb.ru/ .
Ваш путь к удаче: лучшие онлайн казино, посетить.
Попробуйте самые популярные онлайн казино и выигрывайте большие деньги, испытайте прямо сейчас.
Играйте в захватывающие азартные игры в онлайн казино и увеличивайте свой доход, посетите прямо сейчас.
Наслаждайтесь игрой вместе с лучшими онлайн казино, присоединяйтесь прямо сейчас.
Обновленные возможности для любителей азарта в онлайн казино, попробуйте прямо сейчас.
Играть и выигрывать: лучшие онлайн казино для вас, посетите сейчас.
Увлекательные игры и выигрыши в онлайн казино, посетите прямо сейчас.
Большие выигрыши и возможности: лучшие онлайн казино, испытайте сейчас.
Популярные игры и призы в онлайн казино, посетите прямо сейчас.
Лучшие бонусы и выигрыши в онлайн казино, присоединяйтесь прямо сейчас.
Новые возможности и азартные игры в онлайн казино, испытайте прямо сейчас.
Играйте и выигрывайте крупные суммы в самых популярных онлайн казино, испытайте сейчас.
Лучшие игры и призы в онлайн казино, посетите прямо сейчас.
Наши рекомендации: самые популярные онлайн казино, присоединяйтесь сейчас.
Играйте в азартные игры и выигрывайте призы в онлайн казино, попробуйте прямо сейчас.
Лучшие бонусы и выигрыши в онлайн казино, присоединяйтесь прямо сейчас.
Новые возможности и азартные игры в онлайн казино,
онлайн казино онлайн казино .
Выбирайте из самых популярных онлайн казино в Румынии, и стать обладателем крупного выигрыша.
Самые выгодные онлайн казино в Румынии, и стать богаче за считанные минуты.
Выбор казино онлайн для румынских геймеров, где вас ждут невероятные бонусы и акции.
Играйте в онлайн казино из Румынии, для увлекательных игровых приключений.
Лучшие онлайн казино в Румынии на ваш выбор, и получите шанс на крупный джекпот и большие выигрыши.
cazino online gratis https://wla-canvas.ro/ .
Когда заболел мой отец, ему срочно понадобились специальные медицинские приборы. Денег не хватало, а кредитная история у меня была не самой лучшей. Подруга посоветовала Телеграм канал микрозаймы онлайн новые . Она сказала, что там есть малоизвестные займы, которые дают деньги всем по паспорту от 18 лет, и отличная поддержка, которая поможет правильно подать заявку. Оформив займ за 10 минут, я получил 30 тысяч и купил все необходимые приборы. Здоровье отца быстро пошло на поправку. Всем рекомендую этот канал!
На сайте turkhit.tv вы найдете турецкие сериалы онлайн на русском языке. Платформа предлагает огромный выбор сериалов на любой вкус: драмы, комедии, боевики и фэнтези. Все сериалы имеют качественную русскую озвучку, что делает просмотр комфортным и приятным.
На сайте представлены как новинки, так и популярные хиты, такие как “Основание Осман” и “Кровавые цветы”. Платформа не требует регистрации или оплаты, что позволяет наслаждаться любимыми сериалами без лишних хлопот. Заходите на turkhit.tv и наслаждайтесь захватывающими историями.
Онлайн казино с лучшими бонусами и привлекательными акциями
онлайн казино лучшие онлайн казино беларуси .
Всем привет! Может кто знает, где почитатьразные статьи о недвижимости? Сейчас читаю https://gismt72.ru
На нашем сайте вы сможете найти всю необходимую информацию о недвижимости – от бронирования жилья в новостройке до приобретения недвижимости от застройщика.
Мы поможем вам выбрать лучшую квартиру в новостройке, расскажем, как не попасть в ловушку при выборе жилья и подскажем, как сэкономить время и деньги.
Заходите: https://quartz-rsk.ru
vermox 200mg
https://vyzov-santehnika-na-dom.ru.
flomax sale
Приветствую. Может кто знает, где найтиполезные блоги о недвижимости? Сейчас читаю https://kait-volga.ru
Приветствую. Подскажите, где найтиразные статьи о недвижимости? Сейчас читаю https://kaluga-elite.ru
Приветствую. Подскажите, где найтиразные блоги о недвижимости? Пока нашел https://kamenolomnya43.ru
Всем привет! Подскажите, где почитатьразные статьи о недвижимости? Пока нашел https://kmzperm.ru
피망 슬롯 머신
하지만 지금은… 홍지황제도 조조와 같은 문제에 봉착했음을 발견했습니다.
На сайте turkhit.tv можно турецкие сериалы 2023 онлайн. Ежедневно добавляются новые серии в отличном качестве с идеальной русской озвучкой. Здесь вы найдете сериалы всех жанров: от мелодрам до триллеров.
Платформа удобна в использовании и не содержит назойливой рекламы. На turkhit.tv представлены как новинки, так и классические сериалы. Не требуется регистрация или оплата, что делает просмотр еще более приятным. Посетите сайт и наслаждайтесь лучшими турецкими сериалами 2023 года.
Всем привет! Подскажите, где почитатьполезные блоги о недвижимости? Сейчас читаю https://kovry159.ru
Good day! Do you know if they make any plugins to safeguard against hackers?
I’m kinda paranoid about losing everything I’ve worked hard
on. Any suggestions?
Приветствую. Может кто знает, где найтиполезные статьи о недвижимости? Сейчас читаю https://krepegmaster.ru
You are my intake, I have few blogs and sometimes run out from to brand : (.
Приветствую. Может кто знает, где найтиразные статьи о недвижимости? Пока нашел https://kuler-tsentr.ru
Can you be more specific about the content of your article? After reading it, I still have some doubts. Hope you can help me.
Всем привет! Подскажите, где найтиполезные статьи о недвижимости? Сейчас читаю https://liem-com.ru
What Is Sugar Defender? Sugar Defender is a meticulously crafted natural health supplement aimed at helping individuals maintain balanced blood sugar levels. Developed by Jeffrey Mitchell, this liquid formula contains 24 scientifically backed ingredients meticulously chosen to target the root causes of blood sugar imbalances.
акустическое оборудование для актового зала акустическое оборудование для актового зала .
Секреты успешной перетяжки мебели, стильных
Как преобразить интерьер с минимальными затратами, перетянутую мебель мечтали ваши друзья
Сделай свой дом уютным с помощью перетяжки мебели, попробуйте сами
Вдохновляющие идеи для перетяжки мебели, которые понравятся каждому
Перетяжка мебели: секреты мастеров, которые стоит выслушать
перетяжка дивана “КакСвоим”.
Приветствую. Подскажите, где найтиполезные статьи о недвижимости? Сейчас читаю https://oscltd.ru
Приветствую. Может кто знает, где почитатьразные блоги о недвижимости? Пока нашел https://ppu-odk.ru
Understanding NanoDefense Pro: What is it? NanoDefense Pro is a specialized formula designed to improve nail and foot health naturally.
Когда хочется смотреть турецкие сериалы 2024 онлайн на русском языке, turklife.tv становится отличным решением. Здесь вы найдете новейшие сериалы 2024 года в HD 1080 качестве и с превосходной русской озвучкой. Сайт предлагает широкий выбор жанров и удобное разделение по годам.
Каждый день добавляются новые серии, и все это абсолютно бесплатно и без рекламы. Это делает просмотр комфортным и приятным. Turklife.tv – ваш лучший выбор для просмотра турецких сериалов онлайн на русском языке.
Ищете турецкие сериалы новинки? Тогда вам к нам на turkhit.tv! Мы – номер один в Google и Yandex благодаря нашему огромному выбору свежих сериалов. Наслаждайтесь HD качеством и профессиональной русской озвучкой без назойливой рекламы.
Ежедневные обновления и удобный интерфейс делают нас лучшим выбором для любителей турецких сериалов. Присоединяйтесь к нам на turkhit.tv и откройте для себя мир новейших турецких сериалов!
Всем привет! Подскажите, где найтиполезные статьи о недвижимости? Сейчас читаю https://redglade-nn.ru
There’s definately a great deal to learn about this issue.
I like all of the points you’ve made.
Приветствую. Подскажите, где почитатьполезные блоги о недвижимости? Сейчас читаю https://santam1.ru
That is very interesting, You are an overly professional blogger.
I’ve joined your rss feed and sit up for looking for
extra of your wonderful post. Additionally, I’ve shared your site
in my social networks
Hi, I think your site might be having browser compatibility issues.
When I look at your blog site in Opera, it
looks fine but when opening in Internet Explorer, it has some overlapping.
I just wanted to give you a quick heads up! Other then that, excellent blog!
ciprofloxacin
Приветствую. Подскажите, где найтиразные статьи о недвижимости? Пока нашел https://sibarit54.ru
Перетяжка мягкой мебели
https://brest.en.cx/Guestbook/Messages.aspx?page=1&fmode=gb&topic=333133&anchor .
ремонт айфона оригинальные запчасти iphonepochinka.by .
can you purchase diflucan over the counter
Приветствую. Подскажите, где почитатьполезные статьи о недвижимости? Пока нашел https://stroyproektm.ru
Сайт turkhit.tv предлагает большой выбор турецких сериалов для любого вкуса. Здесь можно найти драмы, комедии, боевики, фэнтези и многое другое. Каждый сериал представлен в отличном качестве и с русской озвучкой, что делает просмотр удобным и приятным.
На сайте всегда доступны новинки и популярные сериалы, такие как “Основание Осман” и “Кровавые цветы”. Платформа не требует регистрации или оплаты, что позволяет наслаждаться любимыми сериалами без лишних хлопот. турецкие сериалы онлайн доступны всегда и везде.
buy lasix 40 mg online
Приветствую. Подскажите, где найтиразные блоги о недвижимости? Сейчас читаю https://tent44.ru
Приветствую. Может кто знает, где почитатьразные блоги о недвижимости? Сейчас читаю https://universal37.ru
Write more, thats all I have to say. Literally, it seems as though you relied on the video to make your point. You clearly know what youre talking about, why waste your intelligence on just posting videos to your blog when you could be giving us something enlightening to read?
프라 그마 틱 슬롯 사이트
이 기념관은 내무부와 동시에 전쟁부에 보내질 것입니다.
Merely a smiling visitor here to share the love (:, btw great style and design.
Топ-5 материалов для перетяжки мебели, проверенных временем
Как преобразить интерьер с минимальными затратами, новый взгляд на привычную мебель
Сделай свой дом уютным с помощью перетяжки мебели, попробуйте сами
Тенденции в дизайне мебели для перетяжки, подчеркнут вашу индивидуальность
Как не ошибиться с выбором ткани для перетяжки мебели, которые стоит выслушать
перетяжка дивана “КакСвоим”.
Захватывающий мир онлайн казино, выигрывайте крупные суммы в известных онлайн казино, наслаждайтесь азартом.
Надежность и азарт в онлайн казино, возможность выиграть становится выше.
Эксклюзивные онлайн казино для настоящих азартных игроков, присоединяйтесь и возьмите победу.
Настоящий азарт в онлайн казино, выигрывайте и наслаждайтесь успехом.
Эффективные стратегии в онлайн казино, развивайте навыки и побеждайте.
лучшие онлайн казино на деньги лучшие онлайн казино с минимальным депозитом .
Spot on with this write-up, I seriously believe that this website needs a great deal more attention. I’ll probably be returning to read more, thanks
for the information!
Попробуй свою удачу в 1win казино, выигрывай крупные суммы.
Лучшие игровые автоматы в 1win казино, подарят незабываемый опыт.
1win казино – место, где рождаются победы, играй и получай удовольствие.
Играй и побеждай вместе с 1win казино, получай крупные выигрыши.
1win казино – место, где рождаются победы, получай невероятные эмоции.
Почувствуй адреналин победы в 1win казино, забирай свой джекпот.
1win казино – это мир азарта и фортуны, претворить свои мечты в реальность.
Удовольствие и адреналин в 1win казино, которое ждет тебя прямо сейчас.
1win вход https://luchshiye-onlayn-kazino-rb.com/ .
noroxin pill
I know this web page provides quality dependent content
and additional stuff, is there any other website which offers such stuff
in quality?
Как выбрать лучшую клинику стоматологии, ознакомиться.
Современные технологии в стоматологии, качественный уход за зубами.
Основные причины зубной боли, изучить.
Самые популярные заблуждения о зубах, профессиональные советы стоматолога.
Как избежать проблем с зубами, рекомендуем.
Лечение зубов без боли: реальность или миф?, качественные методики стоматологии.
Что делать при кровоточащих деснах, изучить.
стоматологічна клініка стоматологічна клініка .
Как выбрать лучшие тактичные штаны для активного отдыха, сделанные из качественных материалов.
Выберите стильные тактичные штаны для своего гардероба, которые подчеркнут вашу уверенность и стиль.
Советы по выбору тактичных штанов, для максимального комфорта и функциональности.
Тактичные штаны: идеальное сочетание стиля и практичности, сделанные для динамичного образа жизни.
Тактичные штаны: выбор современного мужчины, и какие модели стоит выбрать для уникального стиля.
тактичні зимові штани тактичні зимові штани .
Как выбрать лучшую клинику стоматологии, изучить.
Уникальные методики лечения зубов, профессиональный уход за зубами.
Эффективные способы обезболивания, предлагаем.
Самые популярные заблуждения о зубах, профессиональные советы стоматолога.
Как избежать проблем с зубами, ознакомиться.
Как выбрать хорошего стоматолога, качественные методики стоматологии.
Что делать при кровоточащих деснах, рекомендуем.
стоматологія допомога стоматологія допомога .
Идеальные тактичные штаны для любого случая, которые подчеркнут вашу индивидуальность.
Новинки в мире тактичной одежды: лучшие штаны, сделанные для вашего комфорта.
Чем отличаются тактичные штаны от обычных, для максимального комфорта и функциональности.
Выберите удобные тактичные штаны для своего гардероба, для стильного и практичного образа.
Тактичные штаны: выбор современного мужчины, для максимального комфорта в походе.
тактичні штани зимові https://vijskovitaktichnishtanu.kiev.ua/ .
Лучшее казино для игры – 1win, не упустите свой шанс!
1win казино – место, где рождаются победы, выигрывайте крупные суммы вместе с 1win казино!
Увлекательное казино 1win ждет вас, получите незабываемые впечатления!
1win казино: ваш путь к легким деньгам, получите удовольствие от азарта!
1win казино: играйте и выигрывайте, присоединяйтесь к победителям!
1win официальный сайт 1win официальный сайт .
Have you ever considered creating an ebook or guest authoring on other websites?
I have a blog based on the same ideas you discuss and would really like to have you share some stories/information. I
know my audience would enjoy your work. If you’re even remotely interested,
feel free to send me an e mail.
where to buy vermox in usa
baclofen brand name in usa
acyclovir capsules 800mg
When I initially commented I clicked the “Notify me when new comments are added” checkbox and now each time a comment is added I get three emails with
the same comment. Is there any way you can remove people from that service?
Thank you!
Приветствую. Подскажите, где почитать разные блоги о недвижимости? Пока нашел https://1eve1.ru
Играйте с удовольствием в 1win казино
1win скачать 1win скачать .
Someone essentially lend a hand to make significantly
posts I would state. This is the very first time I frequented
your website page and to this point? I amazed with the research you made to
create this actual publish extraordinary. Wonderful process!
diflucan otc
Выберите стильные тактичные штаны для повседневной носки, для идеального комфорта и функциональности.
Тактичные штаны: модные тренды этого сезона, для активного образа жизни.
Советы по выбору тактичных штанов, и какие модели стоит обратить внимание.
Тактичные штаны: идеальное сочетание стиля и практичности, для стильного и практичного образа.
Тактичные штаны: выбор современного мужчины, для максимального комфорта в походе.
тактичні штани зимові тактичні штани зимові .
Как выбрать лучшие тактичные штаны для активного отдыха, сделанные из качественных материалов.
Тактичные штаны: модные тренды этого сезона, для активного образа жизни.
Советы по выбору тактичных штанов, и какие модели стоит обратить внимание.
Какие тактичные штаны подойдут именно вам, и какие модели актуальны в этом сезоне.
Какие материалы лучше всего подойдут для тактичных штанов, для максимального комфорта в походе.
купити штани тактичні купити штани тактичні .
Приветствую. Подскажите, где найти разные блоги о недвижимости? Пока нашел https://an72.ru
оснащение конференц зала оснащение конференц зала .
Приветствую. Может кто знает, где почитать полезные блоги о недвижимости? Сейчас читаю https://armid44.ru
В самый неподходящий момент сломалась стиральная машина. Без нее с маленьким ребенком просто не обойтись. Денег на новую машину не было, и кредитная история у меня не идеальная. Вспомнила про Телеграм канал онлайн займы новые мфо . Оказалось, что новые МФО на этом канале дают займы всем, даже с плохой кредитной историей. За 10 минут я оформила займ, и деньги сразу поступили на счет. Благодаря этому займу я смогла быстро купить новую стиральную машину и продолжить заботиться о ребенке без проблем.
Приветствую. Подскажите, где найти разные статьи о недвижимости? Сейчас читаю https://azimut-irkutsk.ru
toradol 20 mg
Как правильно подобрать материал для перетяжки мебели: профессиональные советы и рекомендации, для успешной реализации вашего проекта.
Горячие тенденции в мире перетяжки мебели: эксклюзивные идеи для дома, для создания неповторимого облика вашего дома.
Перетяжка мебели своими руками: идеи для творческого подхода, которые придадут вашему дому неповторимый шарм.
Преимущества перетяжки мебели: почему это стоит попробовать, для создания долговременного и стильного интерьера.
Идеи для выбора профессионала по перетяжке мебели: как не ошибиться, чтобы ваша мебель выглядела идеально.
Перетяжка мебели в стиле минимализм: лаконичные идеи для интерьера, для создания функционального и современного интерьера.
Перетяжка мебели в скандинавском стиле: новые идеи для уютного интерьера, для оформления вашего интерьера в скандинавском духе.
Почему перетяжка мебели является отличным способом экономии: выгодно и стильно, для экономии бюджета и создания стильного дизайна.
Какие расцветки выбрать для перетяжки мебели в провансальском стиле: нежные и пастельные оттенки, для оформления вашего дома в стиле прованс.
Как создать интерьер высокого класса с помощью перетяжки мебели: роскошный подход, для оформления вашего интерьера в стиле элегантности.
Профессиональные секреты перетяжки мебели: как сделать работу максимально эффективной, которые помогут вам сделать правильный выбор и избежать ошибок.
перетяжка мебели в минске перетяжка мебели в минске .
Приветствую. Может кто знает, где почитать разные блоги о недвижимости? Сейчас читаю https://ecn-novodom.ru
Приветствую. Подскажите, где найти полезные статьи о недвижимости? Пока нашел https://germes-alania.ru
Всем привет! Может кто знает, где почитать полезные статьи о недвижимости? Сейчас читаю https://ilinka2.ru
It’s remarkable to visit this site and reading the views of all colleagues concerning this paragraph,
while I am also zealous of getting experience.
видеостена kupit-videostenu.ru .
Hello friends, how is the whole thing, and what you wish for to say concerning this post, in my view its truly awesome designed for me.
Всем привет! Может кто знает, где найти разные блоги о недвижимости? Пока нашел https://kolontaevo-club.ru
baclofen over the counter usa
buy vermox tablets uk
Great article! This is the type of information that should be shared across the net.
Shame on the search engines for not positioning this post upper!
Come on over and talk over with my web site . Thanks =)
ciprofloxacin 750 mg
уличная спортивная площадка купить уличная спортивная площадка купить .
Всем привет! Может кто знает, где найти разные блоги о недвижимости? Пока нашел https://mcsspb.ru
Узнайте всю правду о берцах зсу, происхождение, традиции, погрузитесь в, тайны, Берці зсу: охранители души, истину, погрузитесь, освойте, проникнитесь, традиції, дізнайтеся
купити берці літні зсу https://bercitaktichnizsu.vn.ua/ .
Откройте тайны берців зсу, Какую роль играют берці зсу в обрядах?, Почему берці зсу считаются священными?, значении, Берці зсу: символ верности и чести, тайны, исследуйте, почувствуйте, Берці зсу: подвиги и традиции, Як живеться в берцах зсу, символіку, зрозумійте
літні берці зсу купити літні берці зсу купити .
Amazing issues here. I’m very satisfied to peer your post.
Thank you so much and I’m having a look forward to contact you.
Will you please drop me a mail?
What’s up, its fastidious paragraph about media print, we all be familiar with media
is a wonderful source of information.
Awesome blog you have here but I was curious about if you knew of any forums that cover the
same topics discussed here? I’d really love to be a part of community where I can get responses from other knowledgeable individuals that share the same interest.
If you have any suggestions, please let me know.
Bless you!
Greetings, I do believe your site could possibly be having browser
compatibility problems. When I take a look at your web site
in Safari, it looks fine however, if opening in IE, it has some
overlapping issues. I merely wanted to provide you with
a quick heads up! Apart from that, fantastic site!
It’s wonderful that you are getting thoughts from this post as well as
from our dialogue made here.
It’s awesome in support of me to have a web site, which
is beneficial for my knowledge. thanks admin
ремонт стиральных машин на дому http://www.centr-remonta-stiralnyh-mashin.ru/ .
Comfortable baking margarine: Most recipes call for room temperature butter or margarine,
however this isn’t at all times possible when you have
got determined to bake on the last minute. Now that you realize these 5 helpful ideas,
you possibly can set about baking with out worrying about lacking utensils,
cold margarine, burnt goodies and dry cakes.
Fantastic site. Lots of helpful information here. I am sending it to a few friends ans additionally sharing in delicious. And naturally, thanks to your effort!
Всем привет! Может кто знает, где почитать полезные статьи о недвижимости? Сейчас читаю https://officesaratov.ru
https://qptpcigatqf.kronsberg.info/ .nyKFCMIeqBb
otc retin a
Желаете наслаждаться самыми актуальными сериалами? Сайт turkishclub.tv предлагает новые турецкие сериалы онлайн. У нас вы найдете все новинки турецкого кинематографа в высоком качестве и с профессиональной озвучкой. Без рекламы и с удобной навигацией – идеальный выбор для любителей сериалов.
Присоединяйтесь к нашему сообществу и будьте в курсе всех новинок турецкого телевидения. turkishclub.tv – это ваш лучший источник свежих сериалов, которые можно смотреть онлайн в любое удобное время. Откройте для себя мир турецких сериалов прямо сейчас!
Всем привет! Может кто знает, где найти разные блоги о недвижимости? Сейчас читаю https://sintes21.ru
buy cipro 500
Любите захватывающие истории и динамичные сюжеты? На сайте turkishclub.tv вы найдете турецкие сериалы боевики. У нас собраны самые яркие и увлекательные боевики, доступные для просмотра бесплатно и в высоком качестве 720 HD, с русским переводом и без рекламы.
Наслаждайтесь новыми сериями каждый день и погружайтесь в мир приключений и экшена. Присоединяйтесь к тысячам зрителей, выбравших turkishclub.tv для просмотра лучших турецких боевиков онлайн. Откройте для себя мир захватывающих историй прямо сейчас!
Along with this watering in the night could also be avoided to stop injury to the plants.
Pythium blight can easily be controlled by watering in the day at
the earliest possible time. So this can be a high time to know about the gardening tips for higher maintenance of your lawn. You may easily appreciate the fungus on the top of the lawn as white cotton candy.
A dreadful fungus referred to as Pythium Blight may take its higher hand, if you
happen to leave your lawn wet in the night because this fungus like
to grow in excessive humid situation largely, in the night.
Желаете наслаждаться самыми актуальными сериалами? Сайт turkishclub.tv предлагает новые турецкие сериалы онлайн. У нас вы найдете все новинки турецкого кинематографа в высоком качестве и с профессиональной озвучкой. Без рекламы и с удобной навигацией – идеальный выбор для любителей сериалов.
Присоединяйтесь к нашему сообществу и будьте в курсе всех новинок турецкого телевидения. turkishclub.tv – это ваш лучший источник свежих сериалов, которые можно смотреть онлайн в любое удобное время. Откройте для себя мир турецких сериалов прямо сейчас!
Всем привет! Подскажите, где почитать полезные блоги о недвижимости? Сейчас читаю https://ste96.ru
Всем привет! Может кто знает, где почитатьполезные статьи о недвижимости? Пока нашел https://art-salon-hudojnik.ru
Приветствую. Подскажите, где найтиполезные статьи о недвижимости? Сейчас читаю https://avakan74.ru
Приветствую. Подскажите, где почитатьполезные блоги о недвижимости? Пока нашел https://cks-vrn.ru
Приветствую. Подскажите, где почитать полезные статьи о недвижимости? Пока нашел https://kran-rdk.ru
All this eventually helps in making your body healthy and mentally match.
Workout routines are vital for burning up calories which may have
otherwise accumulated in type of fats around your body.
Your purchasers and prospects are paying on your experience,
time and a spotlight: Be sure they’ve all
three.
Приветствую. Может кто знает, где почитатьразные статьи о недвижимости? Сейчас читаю https://design70.ru
Приветствую. Подскажите, где найтиразные блоги о недвижимости? Пока нашел https://dom-na-kosmonavtov.ru
Всем привет! Подскажите, где найтиразные статьи о недвижимости? Сейчас читаю https://ecofaiber.ru
Всем привет! Подскажите, где найти полезные блоги о недвижимости? Пока нашел https://mart-posters.ru
Всем привет! Может кто знает, где почитатьполезные статьи о недвижимости? Пока нашел https://gavrilov-sergey.ru
Приветствую. Может кто знает, где найтиполезные статьи о недвижимости? Пока нашел https://goncharoff-victory.ru
Всем привет! Подскажите, где почитатьполезные блоги о недвижимости? Пока нашел https://guardian21.ru
Всем привет! Может кто знает, где найтиразные статьи о недвижимости? Сейчас читаю https://jelhouse.ru
Приветствую. Может кто знает, где найти полезные блоги о недвижимости? Сейчас читаю https://metrazhi-omsk.ru
Приветствую. Может кто знает, где найтиразные статьи о недвижимости? Пока нашел https://jkfontani.ru
Приветствую. Подскажите, где найтиполезные статьи о недвижимости? Пока нашел https://keramoff-plitka.ru
Всем привет! Может кто знает, где почитать разные статьи о недвижимости? Пока нашел https://tochkacn.ru
Всем привет! Может кто знает, где почитатьразные статьи о недвижимости? Сейчас читаю https://kraftmanpro.ru
Приветствую. Может кто знает, где найтиразные блоги о недвижимости? Пока нашел https://legatinvest.ru
Всем привет! Может кто знает, где найти полезные блоги о недвижимости? Пока нашел https://mik-dom.ru
Окна недорого в Иркутске fod38.ru
По теме установка окон иркутск мы обязательно Вам окажем помощь. Окна от нашей фабрики являются экологичными, так как в них не содержится свинец. После установки, в помещениях будет бесшумно и спокойно, а также надежно для детей, ведь мы делаем ручки с замком. Все окна с защитой УФ, а также их легко мыть, комфортно проветривать и красиво на них смотреть.
Всем привет! Может кто знает, где найтиразные блоги о недвижимости? Сейчас читаю https://lestnicy-ok.ru
Всем привет! Может кто знает, где найтиразные статьи о недвижимости? Сейчас читаю https://likolordom.ru
Всем привет! Может кто знает, где почитатьразные блоги о недвижимости? Сейчас читаю https://modul724.ru
Всем привет! Подскажите, где найтиразные блоги о недвижимости? Сейчас читаю https://mtdis.ru
Приветствую. Подскажите, где найти полезные блоги о недвижимости? Сейчас читаю https://miro-teh-ural.ru
Всем привет! Может кто знает, где почитатьполезные статьи о недвижимости? Сейчас читаю https://muhoedovo.ru
Приветствую. Может кто знает, где почитатьполезные блоги о недвижимости? Сейчас читаю https://obereg-uv.ru
Всем привет! Подскажите, где почитатьполезные статьи о недвижимости? Сейчас читаю https://psfasad.ru
Купить окна ПВХ в Иркутске fod38.ru
По вопросу ремонт пластиковых окон в иркутске мы непременно Вам поможем. Окна от нашей фабрики являются экологически чистыми, так как в них не используется свинец. После установки, в комнате будет бесшумно и комфортно, а также безопасно для детей, ведь мы устанавливаем ручки с замком. Все стекла с защитой от ультрафиолета, а также их легко мыть, удобно проветривать и они впишутся в любой дизайн.
Приветствую. Может кто знает, где найтиразные блоги о недвижимости? Сейчас читаю https://sbitstroyservis.ru
I quite like reading a post that will make men and women think.
Also, thank you for permitting me to comment!
Приветствую. Подскажите, где найти разные блоги о недвижимости? Сейчас читаю https://mzhk-stroy.ru
Всем привет! Может кто знает, где найтиразные статьи о недвижимости? Пока нашел https://septik-baikal.ru
Всем привет! Подскажите, где почитатьполезные блоги о недвижимости? Сейчас читаю https://solopetersburg.ru
Всем привет! Подскажите, где найтиразные статьи о недвижимости? Сейчас читаю https://studiocolors-nsk.ru
Приветствую. Подскажите, где найтиполезные блоги о недвижимости? Пока нашел https://tuimaada-i.ru
Приветствую. Подскажите, где найти полезные статьи о недвижимости? Пока нашел https://nagaevodom.ru
Making a chart of your objectives and put stars or stickers on it when you obtain them.
You have spent the majority of your life working onerous, sacrificing and making
great selections for your self, and others, if you’ve
raised a household. Something tells me I might need to watch for my 60th
birthday. Mechanics should take away many parts to get into the timing system, and the belt alternative can easily run over $1,000
with labor. Medication has come a long way
through the years.
Всем привет! Подскажите, где почитатьполезные статьи о недвижимости? Сейчас читаю https://ventiliatsya-volgograd.ru
Всем привет! Подскажите, где почитатьразные статьи о недвижимости? Сейчас читаю https://yugserv3.ru
I wanted to thank you for this great read!! I definitely enjoying every little bit of it I have you bookmarked to check out new stuff you post…
Приветствую. Может кто знает, где почитатьразные блоги о недвижимости? Сейчас читаю https://zkvartal5.ru
Приветствую. Подскажите, где найти полезные блоги о недвижимости? Сейчас читаю https://potolkinomer1.ru
Приветствую. Может кто знает, где почитатьполезные блоги о недвижимости? Пока нашел https://z-sip.ru
Привет! Устали от отказов и высоких процентов? Наш канал – это то, что вам нужно! Мы собрали только те МФО, которые предлагают займы под 0% и с процентной ставкой не выше 0.8% в день. Даже если у вас есть просрочки по кредитам и плохая кредитная история, вы сможете получить деньги без проблем. У нас также есть круглосуточная поддержка и советы для заемщиков. Подписывайтесь и решите свои финансовые проблемы быстро и легко!
Приветствую. Подскажите, где найти полезные блоги о недвижимости? Сейчас читаю https://promresmag.ru
cheap advair diskus
Всем привет! Подскажите, где почитать полезные статьи о недвижимости? Сейчас читаю https://santech31.ru
Приветствую. Может кто знает, где почитатьразные блоги о недвижимости? Сейчас читаю https://z-sip.ru
Hey there! I know this is kinda off topic but I’d figured I’d ask. Would you be interested in trading links or maybe guest authoring a blog post or vice-versa? My website discusses a lot of the same topics as yours and I feel we could greatly benefit from each other. If you happen to be interested feel free to shoot me an email. I look forward to hearing from you! Fantastic blog by the way!
Всем привет! Подскажите, где почитать разные статьи о недвижимости? Пока нашел https://santex-expert.ru
Приветствую. Подскажите, где почитатьразные статьи о недвижимости? Пока нашел https://z-sip.ru
Всем привет! Подскажите, где найтиразные статьи о недвижимости? Сейчас читаю https://z-sip.ru
Всем привет! Может кто знает, где почитатьразные статьи о недвижимости? Пока нашел https://z-sip.ru
wow mythic raid carry wow mythic raid carry .
cheap baclofen online
Приветствую. Подскажите, где найтиполезные блоги о недвижимости? Пока нашел https://z-sip.ru
Приветствую. Подскажите, где найти разные блоги о недвижимости? Сейчас читаю https://schuconvr.ru
Всем привет! Может кто знает, где почитатьполезные блоги о недвижимости? Сейчас читаю https://z-sip.ru
Приветствую. Может кто знает, где найтиполезные блоги о недвижимости? Пока нашел https://z-sip.ru
Всем привет! Подскажите, где найтиполезные блоги о недвижимости? Сейчас читаю https://z-sip.ru
Всем привет! Может кто знает, где найти полезные блоги о недвижимости? Сейчас читаю https://simposad.ru
Приветствую. Может кто знает, где почитатьразные блоги о недвижимости? Пока нашел https://z-sip.ru
This web page was last edited on 12 April 2024, at 22:28 (UTC).
Specifically clown contouring which was throughout Instagram for the last two weeks, but
we’ll squeeze these two as they share the identical method however
totally different aesthetics.
Всем привет! Подскажите, где найтиразные блоги о недвижимости? Сейчас читаю https://z-sip.ru
Всем привет! Подскажите, где почитатьразные статьи о недвижимости? Сейчас читаю https://z-sip.ru
Приветствую. Подскажите, где найти полезные статьи о недвижимости? Пока нашел https://smgarant.ru
Everything is very open and very clear explanation of issues. was truly information.Seo Paketi Skype: By_uMuT@KRaLBenim.Com -_- live:by_umut
After all, what a great site and informative posts, I will upload inbound link – bookmark this web site? Regards, Reader.Seo Paketi Skype: By_uMuT@KRaLBenim.Com -_- live:by_umut
Good info. Lucky me I reach on your website by accident, I bookmarked it. Seo Paketi Skype: By_uMuT@KRaLBenim.Com -_- live:by_umut
Thank you great posting about essential oil. Hello Administ . Seo Paketi Skype: By_uMuT@KRaLBenim.Com -_- live:by_umut
After all, what a great site and informative posts, I will upload inbound link – bookmark this web site? Regards, Reader.Seo Paketi Skype: By_uMuT@KRaLBenim.Com -_- live:by_umut
Hi, just required you to know I he added your site to my Google bookmarks due to your layout. But seriously, I believe your internet site has 1 in the freshest theme I??ve came across.Seo Paketi Skype: By_uMuT@KRaLBenim.Com -_- live:by_umut
Thank you great posting about essential oil. Hello Administ . Seo Paketi Skype: By_uMuT@KRaLBenim.Com -_- live:by_umut
Everything is very open and very clear explanation of issues. was truly information.Seo Paketi Skype: By_uMuT@KRaLBenim.Com -_- live:by_umut
I really love to read such an excellent article. Helpful article. Hello Administ . Seo Paketi Skype: By_uMuT@KRaLBenim.Com -_- live:by_umut
Nice article inspiring thanks. Hello Administ . Seo Paketi Skype: By_uMuT@KRaLBenim.Com -_- live:by_umut
사이트 토토
Zhu Houzhao는 주저하지 않고 먼저 상처에 약을 바르고 붕대를 감았습니다.
Всем привет! Подскажите, где почитатьразные блоги о недвижимости? Пока нашел https://z-sip.ru
Приветствую. Может кто знает, где почитать полезные статьи о недвижимости? Пока нашел https://stilnyjpol.ru
Приветствую. Подскажите, где почитатьполезные блоги о недвижимости? Пока нашел https://z-sip.ru
When I originally commented I clicked the “Notify me when new comments are added” checkbox and now each time a comment
is added I get three emails with the same comment. Is there any way you can remove
me from that service? Bless you!
Всем привет! Подскажите, где найтиразные блоги о недвижимости? Пока нашел https://z-sip.ru
Приветствую. Подскажите, где найти полезные блоги о недвижимости? Пока нашел https://tc-all.ru
I love your blog.. very nice colors & theme. Did you
make this website yourself or did you hire someone to do it for you?
Plz respond as I’m looking to create my own blog and would like
to find out where u got this from. thanks a lot
Приветствую. Подскажите, где почитатьразные блоги о недвижимости? Сейчас читаю https://z-sip.ru
Всем привет! Может кто знает, где найтиполезные блоги о недвижимости? Сейчас читаю https://z-sip.ru
Всем привет! Может кто знает, где найти разные статьи о недвижимости? Пока нашел https://teplohod-denisdavidov.ru
Всем привет! Может кто знает, где найтиполезные статьи о недвижимости? Сейчас читаю https://z-sip.ru
It’s awesome to pay a visit this web page and reading the views of all friends regarding this paragraph, while I
am also keen of getting experience.
Приветствую. Подскажите, где почитатьполезные блоги о недвижимости? Сейчас читаю https://z-sip.ru
Приветствую. Может кто знает, где почитать полезные статьи о недвижимости? Сейчас читаю https://titovloft.ru
Приветствую. Подскажите, где найти полезные статьи о недвижимости? Пока нашел https://toadmarket.ru
Всем привет! Подскажите, где почитатьполезные статьи о недвижимости? Сейчас читаю https://z-sip.ru
Всем привет! Может кто знает, где почитать полезные блоги о недвижимости? Пока нашел https://u-mechanik.ru
Всем привет! Подскажите, где почитать разные блоги о недвижимости? Сейчас читаю https://utc96.ru
Приветствую. Подскажите, где найти полезные статьи о недвижимости? Пока нашел https://vortex-los.ru
Приветствую. Подскажите, где почитатьразные блоги о недвижимости? Пока нашел https://z-sip.ru
My brother suggested I might like this blog. He was entirely right.
This post actually made my day. You can not imagine just how much time I had
spent for this info! Thanks!
Приветствую. Подскажите, где почитать полезные статьи о недвижимости? Сейчас читаю https://yah-bomag.ru
Приветствую. Может кто знает, где почитатьполезные статьи о недвижимости? Сейчас читаю https://z-sip.ru
nolvadex 10mg online
Всем привет! Может кто знает, где найти полезные статьи о недвижимости? Пока нашел https://yaoknaa.ru
Всем привет! Может кто знает, где найтиразные статьи о недвижимости? Сейчас читаю https://z-sip.ru
Приветствую. Может кто знает, где найтиполезные статьи о недвижимости? Сейчас читаю https://art-salon-hudojnik.ru
Приветствую. Подскажите, где почитать полезные статьи о недвижимости? Пока нашел https://zt365.ru
Приветствую. Может кто знает, где почитатьразные блоги о недвижимости? Пока нашел https://avakan74.ru
Howdy! I’m at work browsing your blog from my new
apple iphone! Just wanted to say I love reading through your blog and look forward to all your posts!
Keep up the great work!
По части факоэмульсификация мы Вам можем помочь. У нас широкий выбор услуг: метод коррекции зрения ласик, методика проведения операции ФРК, оперативное лечение катаракты, операция склеропластика, ортокератологические линзы, безоперационная блефаропластика аппаратом JETT PLASMA LIFT и многие другие. Приходите за квалифицированной консультацией к нашим врачам.
Всем привет! Может кто знает, где почитатьразные блоги о недвижимости? Сейчас читаю https://cks-vrn.ru
Всем привет! Подскажите, где почитатьполезные статьи о недвижимости? Пока нашел https://z-sip.ru
Twenty-three of the primary 30 books have been written by a
journalist named Mildred Wirt Benson, beneath the route of Edward Stratemeyer, who developed
several sequence books for youngsters (Ever learn the Hardy Boys, Bobbsey Twins
or Tom Swift? These have been his creations too.) Stratemeyer got here up with the characters and
outlines and farmed out the content material to varied ghostwriters to
complete. To understand Nest’s value, let’s first look at what other thermostats do.
Всем привет! Может кто знает, где почитать полезные блоги о недвижимости? Пока нашел https://astali.ru
Всем привет! Может кто знает, где почитатьразные статьи о недвижимости? Пока нашел https://design70.ru
Great post thank you. Hello Administ . Seo Paketi Skype: By_uMuT@KRaLBenim.Com -_- live:by_umut
Everything is very open and very clear explanation of issues. was truly information.Seo Paketi Skype: By_uMuT@KRaLBenim.Com -_- live:by_umut
Hello! I could have sworn I’ve been to this blog before but after browsing through some of the post I realized it’s new to me.Seo Paketi Skype: By_uMuT@KRaLBenim.Com -_- live:by_umut
Everything is very open and very clear explanation of issues. was truly information.Seo Paketi Skype: By_uMuT@KRaLBenim.Com -_- live:by_umut
Great post thank you. Hello Administ . Seo Paketi Skype: By_uMuT@KRaLBenim.Com -_- live:by_umut
Everything is very open and very clear explanation of issues. was truly information.Seo Paketi Skype: By_uMuT@KRaLBenim.Com -_- live:by_umut
Hello to every , as I am in fact keen of reading this blog’s post to be updated
daily. It carries good stuff.
Thank you for great content. Hello Administ. Seo Paketi Skype: By_uMuT@KRaLBenim.Com -_- live:by_umut
Hi, just required you to know I he added your site to my Google bookmarks due to your layout. But seriously, I believe your internet site has 1 in the freshest theme I??ve came across.Seo Paketi Skype: By_uMuT@KRaLBenim.Com -_- live:by_umut
Hello! I could have sworn I’ve been to this blog before but after browsing through some of the post I realized it’s new to me.Seo Paketi Skype: By_uMuT@KRaLBenim.Com -_- live:by_umut
Всем привет! Может кто знает, где почитатьполезные статьи о недвижимости? Сейчас читаю https://z-sip.ru
I really love to read such an excellent article. Helpful article. Hello Administ . Seo Paketi Skype: By_uMuT@KRaLBenim.Com -_- live:by_umut
Приветствую. Может кто знает, где почитатьполезные статьи о недвижимости? Сейчас читаю https://dom-na-kosmonavtov.ru
Всем привет! Может кто знает, где почитать разные блоги о недвижимости? Сейчас читаю https://batstroimat24.ru
Nice article inspiring thanks. Hello Administ . Seo Paketi Skype: By_uMuT@KRaLBenim.Com -_- live:by_umut
Hello! I could have sworn I’ve been to this blog before but after browsing through some of the post I realized it’s new to me.Seo Paketi Skype: By_uMuT@KRaLBenim.Com -_- live:by_umut
Всем привет! Подскажите, где почитатьразные блоги о недвижимости? Сейчас читаю https://ecofaiber.ru
As I have mentioned earlier, blog comments initiate a discuss between the
network marketing coach and the viewers.If you aren’t going to
reply to every remark that you simply obtain, you won’t be able to hold a sociable dialogue
together with your followers. You may win the attention of your readers
if you are going for motivating articles.
It wants your time, dedication, persistence and attention.
Всем привет! Может кто знает, где почитатьразные блоги о недвижимости? Сейчас читаю https://z-sip.ru
Всем привет! Подскажите, где найтиполезные статьи о недвижимости? Пока нашел https://gavrilov-sergey.ru
Приветствую. Может кто знает, где почитать разные блоги о недвижимости? Сейчас читаю https://bdrsu-2.ru
Всем привет! Подскажите, где найтиполезные статьи о недвижимости? Пока нашел https://z-sip.ru
В отношении коррекция методом ласик мы Вам поможем. У нас большой спектр услуг: метод коррекции зрения суперласик, лазерная коагуляция сетчатки, оперативное лечение глакуомы, лазерная дисцизия задней капсулы хрусталика, ортокератологические линзы, лифтинг век JETT PLASMA LIFT и многие другие. Обратитесь за профессиональной помощью к нашим специалистам.
Nice article inspiring thanks. Hello Administ . Seo Paketi Skype: By_uMuT@KRaLBenim.Com -_- live:by_umut
Nice article inspiring thanks. Hello Administ . Seo Paketi Skype: By_uMuT@KRaLBenim.Com -_- live:by_umut
Приветствую. Подскажите, где найтиразные блоги о недвижимости? Сейчас читаю https://guardian21.ru
Всем привет! Подскажите, где почитать разные статьи о недвижимости? Пока нашел https://centro-kraska.ru
Всем привет! Может кто знает, где найтиполезные статьи о недвижимости? Пока нашел https://jelhouse.ru
order bactrim ds
Всем привет! Подскажите, где найтиразные блоги о недвижимости? Пока нашел https://jkfontani.ru
Приветствую. Может кто знает, где найти полезные блоги о недвижимости? Сейчас читаю https://cvetkrovli.ru
Всем привет! Может кто знает, где найтиразные блоги о недвижимости? Сейчас читаю https://keramoff-plitka.ru
Mediaget – это не просто программа, а целая экосистема для работы с цифровым контентом. Помимо основного приложения для ПК, пользователям доступны мобильные версии для iOS и Android, позволяющие управлять загрузками на ходу. Кроме того, Mediaget предлагает интеграцию с популярными облачными хранилищами, что позволяет легко синхронизировать и хранить загруженные файлы. Особого внимания заслуживает веб-интерфейс Mediaget, доступный по адресу https://skachat-mediaget-plus.ru, который обеспечивает полный контроль над загрузками с любого устройства, имеющего доступ к интернету. Эта функция особенно полезна для пользователей, которые часто работают удаленно или используют несколько устройств. Веб-интерфейс также предлагает расширенную аналитику и статистику загрузок, помогая оптимизировать использование программы.
медиагет скачать
медиа гет скачать
медиагет скачать бесплатно
Приветствую. Может кто знает, где найтиполезные статьи о недвижимости? Сейчас читаю https://z-sip.ru
Всем привет! Подскажите, где почитатьполезные блоги о недвижимости? Пока нашел https://kraftmanpro.ru
Всем привет! Может кто знает, где почитать разные блоги о недвижимости? Сейчас читаю https://deon-stroy.ru
Всем привет! Подскажите, где почитатьполезные блоги о недвижимости? Пока нашел https://legatinvest.ru
Приветствую. Подскажите, где найтиразные статьи о недвижимости? Пока нашел https://z-sip.ru
This is a topic close to my heart cheers, where are your contact details though?
Приветствую. Может кто знает, где найтиразные статьи о недвижимости? Пока нашел https://lestnicy-ok.ru
We’d even know two or three of them already — but we aren’t telling.
Two predominant areas of focus are the person’s arms and legs.
There are two essential methods to regulate the intensity.
The water jets precipitated the waterproof membrane to distend and stretch in methods Arzt had
not supposed. There are so many ways to be good, but for day-to-day life and enterprise, some frequent sense is a must.
However there are other causes for a bride to put on white.
The park’s dark skies are an ideal stage for clear
views of the Milky Method galaxy.S. Spheres (even if
they don’t seem to be perfect) make bubbles.
But how do you make a device that squeezes a user without
turning it into a harmful machine better fitted to a horror
film? If you want to see the sites in Santa Monica and Napa Valley, make
the lodge reservations in those areas.
Mediaget выделяется среди других торрент-клиентов своим инновационным подходом к организации загрузок. Программа использует передовые алгоритмы машинного обучения для оптимизации процесса скачивания, анализируя паттерны сетевого трафика и поведение пиров. Это позволяет Mediaget автоматически настраивать параметры загрузки для достижения максимальной эффективности. Кроме того, уникальная функция “умного кэширования” предугадывает, какие части файла будут востребованы в первую очередь, ускоряя доступ к контенту еще до завершения загрузки. Пользователи, заинтересованные в глубоком понимании этих технологий, могут ознакомиться с подробным техническим описанием на странице https://skachat-mediaget-online.ru, где разработчики раскрывают детали используемых алгоритмов и делятся результатами внутренних тестов производительности.
скачать mediaget на пк
mediaget скачать
медиа гет скачать
Всем привет! Подскажите, где почитать полезные блоги о недвижимости? Сейчас читаю https://dom-vasilevo.ru
For example, children, older adults, and individuals
with pre-existing psychological health situations could also be
more inclined to the damaging effects of polluted air on temper and emotional nicely-being.
By creating healthy attachment kinds, people can build stronger connections and
experience higher satisfaction in their relationships. WHO has
known as for the event of revolutionary strategies to deal with these nonetheless-rampant diseases, and continues to
fund research into creating effective vaccines. The agreement, called Framework Convention on Tobacco Management, attempts to restrict tobacco promoting, sponsorship, and promotion;
set up labeling controls; set up indoor “clear air” controls; and scale back
tobacco smuggling. BioShock is considered one among last generation’s best video games and
would make an excellent framework for a blockbuster movie.
The pigeon’s just one instance of an animal some humans eat that is probably smarter
than your pet kitty or guinea pig. Scientists also have performed checks showing that pigs
can immediately be taught to comply with each other when they think one other
pig is aware of the placement of meals. Why think about
pig brains once we can be excited about consuming a ham sandwich?
Всем привет! Может кто знает, где найтиполезные блоги о недвижимости? Пока нашел https://likolordom.ru
Freshmen at all times need help from the tour-operator in order that the journey may be
nicely planned and executed in a secure method.
How Do You Prepare For A Camping Journey? South Australia Department for Transport, Power and Infrastructure.
There are many selections and options for evening dinning however if
you combine the friendliness of the south with the tradition of Latin America, you’re certain to seek out an evening of great dining, dancing, and leisure.
Therefore, what are you waiting for? Concept’s all well and good,
but the highway calls so that you can make sure the lights are working in apply.
Preserving your trailer properly maintained entails keeping your
trailer’s lights in correct working order. Ask your helper to confirm each is working earlier than transferring on to the subsequent light.
You may also dab this type of grease around mild bulb sockets and other places where
moisture can get into your electrical system.
Всем привет! Подскажите, где найтиполезные блоги о недвижимости? Пока нашел https://modul724.ru
Всем привет! Может кто знает, где почитатьполезные блоги о недвижимости? Пока нашел https://mtdis.ru
Всем привет! Подскажите, где почитатьполезные блоги о недвижимости? Сейчас читаю https://z-sip.ru
Всем привет! Может кто знает, где почитатьразные статьи о недвижимости? Сейчас читаю https://muhoedovo.ru
Relaxation is the alternative of tension, so his work led to the usage of the
word “calm down” to explain the act of turning into much less tense, anxious, or careworn. The Civil Rights Act of 1964… During the 1970s, medical institutions acknowledged relaxation strategies such
as progressive muscle relaxation as protected and effective
alternate options to drug remedies for certain conditions
like anxiety, insomnia, and hypertension. Remedies embody the resort’s after
a long day’s clambering around Hue’s ancient citadel or
the Nguyen tombs. Progressive muscle relaxation might be effectively used with other modern medical
therapies or different complementary therapies
that promote well being. Progressive muscle relaxation is
utilized in some ways. Progressive muscle relaxation goals to
reverse these physique states back to more neutral, relaxed states.
When the muscle tension is launched, attention is directed in the direction of the differences felt
throughout tension and relaxation so that the affected person learns to recognize
the distinction between the states. In 1929, Jacobson published the book Progressive Relaxation, which included an in depth procedure for eradicating tension in the muscles.
The person can attempt to visualize how the tension looks like and how it is slowly fading out of their body.
buy raid carry wow https://kreativwerkstatt-esens.de/ .
It was officially proclaimed a settlement on Feb.
7, 1788. Nevertheless, this was not the primary time that folks had come to explore
Australia. Right here you too can explore the Tombs made
within the 14th century. With their intensive collection of clothing,
accessories, and jewelry, you possibly can create a really one-of-a-form and edgy look
that showcases your particular person style.
Since these are the two predominant characteristics most of
us look for in tomatoes, it pays to eat them sooner quite than later.
It achieved its major cartographic goals and succeeded in exploring the huge area,
drawing accurate charts of previously unexplored coastlines and fjords, naming numerous geographic features, and
gathering a wealth of scientific data. With exploration that started throughout the European Renaissance,
data of the Earth’s floor accumulated quickly, such that many of the world’s coastlines had been mapped, at
least roughly, by the mid-1700s and the continental interiors by the twentieth century.
It’s compulsory to attend while you obtain a summons, so not less than there is a bright side figuring out you
may be compensated for the times taken from work.
Consecutive days of climbing a mountain and camping are very difficult.
Всем привет! Может кто знает, где найтиразные блоги о недвижимости? Сейчас читаю https://z-sip.ru
Приветствую. Подскажите, где найтиразные статьи о недвижимости? Сейчас читаю https://obereg-uv.ru
Приветствую. Подскажите, где почитатьразные статьи о недвижимости? Пока нашел https://psfasad.ru
Всем привет! Может кто знает, где найтиполезные статьи о недвижимости? Пока нашел https://sbitstroyservis.ru
Всем привет! Может кто знает, где найтиполезные статьи о недвижимости? Пока нашел https://septik-baikal.ru
Приветствую. Подскажите, где найтиразные блоги о недвижимости? Пока нашел https://z-sip.ru
Приветствую. Подскажите, где почитатьразные блоги о недвижимости? Пока нашел https://solopetersburg.ru
dexona tablet price
Приветствую. Подскажите, где почитатьполезные статьи о недвижимости? Сейчас читаю https://studiocolors-nsk.ru
Приветствую. Может кто знает, где почитатьполезные статьи о недвижимости? Пока нашел https://z-sip.ru
Всем привет! Может кто знает, где найтиполезные статьи о недвижимости? Сейчас читаю https://tuimaada-i.ru
Всем привет! Подскажите, где найтиполезные блоги о недвижимости? Пока нашел https://z-sip.ru
Приветствую. Подскажите, где почитатьполезные блоги о недвижимости? Пока нашел https://ventiliatsya-volgograd.ru
dexamethasone 4 mg tablet india
ciprofloxacin 50 mg
Всем привет! Может кто знает, где почитатьразные статьи о недвижимости? Сейчас читаю https://yugserv3.ru
bactrim tablet india
Wonderful web site. Lots of helpful info here. I am sending it to several friends ans also sharing in delicious. And of course, thank you for your sweat!
I have been examinating out a few of your stories and i can state pretty clever stuff. I will definitely bookmark your website.
Приветствую. Может кто знает, где почитатьполезные статьи о недвижимости? Пока нашел https://zkvartal5.ru
100mg baclofen
lasix 25 mg
I simply couldn’t depart your website before suggesting that
I really enjoyed the standard info a person provide in your visitors?
Is gonna be again ceaselessly in order to check out new posts
strattera
Всем привет! Может кто знает, где найтиразные блоги о недвижимости? Пока нашел https://7832206.ru
Защитите свои данные с помощью резидентских прокси, рекомендуем этим инструментом.
В чем особенность резидентских прокси?, ознакомьтесь с подробностями.
Какой резидентский прокси выбрать?, инструкция для пользователей.
Зачем нужны резидентские прокси?, ознакомьтесь с возможностями.
Как резидентские прокси обеспечивают безопасность?, обзор функций безопасности.
Защита от каких угроз обеспечивает резидентский прокси?, анализируем важные аспекты.
Какие преимущества дает использование резидентских прокси?, проанализируем основные плюсы.
Как быстрее работать в сети с резидентским прокси?, советы для оптимизации работы.
Зачем использовать резидентский прокси для сбора информации?, обзор возможностей для парсеров.
Как оставаться анонимным в Интернете с резидентским прокси, практические шаги к безопасности онлайн.
Секреты эффективной работы в соцсетях с резидентским прокси, подробный обзор функционала.
Как сэкономить время с помощью аренды резидентского прокси?, проанализируем лучшие варианты.
Как избежать DDoS с резидентским прокси?, рассмотрим меры безопасности.
Какие преимущества привлекают пользователей к резидентским прокси?, подробно изучим основные факторы.
Как выбрать между резидентским и дата-центровым прокси?, рекомендации для выбора.
резидентский прокси сервер https://rezidentnieproksi.ru/ .
Всем привет! Может кто знает, где найти разные блоги о недвижимости? Сейчас читаю https://2204000.ru
Всем привет! Подскажите, где найтиполезные блоги о недвижимости? Сейчас читаю https://acc-sib.ru
Всем привет! Может кто знает, где найти полезные статьи о недвижимости? Пока нашел https://adeldv.ru
슬롯 커뮤
그런데 이번에 그들이 가져온 것은 야멘에서 공문서였다.
Безопасность данных с резидентскими прокси, как это работает.
Смотрите зарубежные сериалы с резидентскими прокси, полномасштабным контентом.
Увеличьте скорость и стабильность интернет-соединения с резидентскими прокси, как это работает.
Защитите свои учетные данные и личную информацию с резидентскими прокси, и чувствуйте себя спокойно.
Прячьте свою локацию и IP-адрес с резидентскими прокси, и наслаждайтесь анонимностью.
Скачивайте файлы анонимно через резидентские прокси, и не опасайтесь за свою приватность.
прокси резидентные https://rezidentnie-proksi.ru/ .
Приветствую. Может кто знает, где почитатьразные статьи о недвижимости? Сейчас читаю https://aladrom.ru
Приветствую. Подскажите, где найти полезные статьи о недвижимости? Сейчас читаю https://eniseynev.ru
Great site you have here.. It’s difficult to find quality writing like
yours these days. I seriously appreciate people like you! Take
care!!
I’m amazed, I must say. Rarely do I encounter a blog that’s equally educative and amusing, and
without a doubt, you’ve hit the nail on the head.
The problem is an issue that too few folks are speaking intelligently about.
I’m very happy I came across this in my hunt for something relating
to this.
Good site! I really love how it is easy on my eyes and the data are well written. I am wondering how I could be notified when a new post has been made. I have subscribed to your RSS feed which must do the trick! Have a great day!
Ставки на спорт с высокими коэффициентами | Надежные ставки на 1win | 1win дает возможность выиграть крупный приз | На 1win вы всегда в плюсе| Начни выигрывать с 1win| Побеждайте с 1win| 1win – платформа для успешных ставок| Стань частью команды 1win| 1win поможет вам стать чемпионом| 1win – это ваш верный партнер в ставках
1win вход 1win вход .
Приветствую. Может кто знает, где почитатьразные статьи о недвижимости? Сейчас читаю https://allianceplast.ru
Всем привет! Подскажите, где найти полезные статьи о недвижимости? Сейчас читаю https://fuseitdecore.ru
Согласование перепланировки в здании в Москве — это настоящее испытание для тех, кто любит острые ощущения. Хотите почувствовать себя героем квеста? Тогда вам точно к нам!
Мы с радостью возьмем на себя все сложности этого увлекательного процесса. Наша команда профессионалов поможет вам пройти все этапы и получить заветные разрешения. Ведь кто еще, как не мы, знает, как сделать бюрократию чуть более «дружелюбной»?
1win – ваш идеальный партнер для ставок
Удача всегда на вашей стороне с 1win
Попробуйте свои силы на платформе 1win
1win – надежный партнер для всех любителей ставок
Букмекерская контора 1win радует своих клиентов каждый день
Ваши ставки всегда успешные с 1win
Ставки на спорт с 1win – высокие коэффициенты и увлекательные матчи
1win гарантирует вам только лучшие условия для ставок
Увеличьте свои шансы на успех с букмекерской конторой 1win
1win: ваш выбор номер один в мире ставок
Ставки на спорт никогда не были такими увлекательными как с 1win
1win делает вашу игру более прибыльной и увлекательной
1win – это ваша возможность побеждать
1win всегда на вашей стороне|Получайте удовольствие от ставок с 1win
1win гарантирует вам качественный сервис и высокие шансы на успех|Увлекательные ставки и азартные игры на платформе 1win|1win – ваш верный партнер в мире ставок|1win – ваш проводник в мире ставок и азарта|Играйте и выигрывайте с 1win|1win делает вашу игру максимально увлекательной и выгодной|1win – ваш путь к успеху и богатству|Ваши ставки всегда успешные с 1win|1win делает вашу игру более прибыльной и интересной|1win – это ваш шанс стать победителем|1win – ваш партнер в мире ставок и азарта|Увеличивайте свои шансы на успех с 1win|1win – это ваш ключ к финансовой стабильности|Сделайте свои ставки более увлекательными с 1win|1win гарантирует вам только выигрышные ставки|Начните свой путь к успеху с 1win|Присоединяйтесь к лидерам ставок на 1win|Ув
1win зеркало https://1win-ofitsialnyy.by/ .
Приветствую. Подскажите, где найтиполезные статьи о недвижимости? Сейчас читаю https://anc-k.ru
Всем привет! Подскажите, где найти разные блоги о недвижимости? Сейчас читаю https://galastroy-sk.ru
Всем привет! Подскажите, где почитатьразные статьи о недвижимости? Сейчас читаю https://aprofit-vlg.ru
Приветствую. Подскажите, где найти разные блоги о недвижимости? Пока нашел https://ggs45.ru
Купить дом в Ижевске нк18.рф
По теме строительство монолитных домов вы на правильном пути. Здесь можно купить и заехать в дом за срок от 8 месяцев, взять ипотеку на выгодных условиях, и не проиграть в средствах — цена по время строительства не поменяется. Мы уже большое количество лет на рынке и имеем положительный опыт в архитектуре, кроме этого, всегда совершенствуемся, изучаем новинки и стараемся быть лучше с каждым построенным домом. Дается увеличенная гарантия на кровлю, фундамент и стены.
Very good article. I absolutely appreciate this site.
Stick with it!
Ставки на спорт в 1win: высокие коэффициенты и большие выигрыши, советуем.
Играйте и выигрывайте вместе с 1win, проверить свои навыки.
1win: быстрый и удобный способ заработать деньги, предлагаем.
Ставки на киберспорт: лучшие коэффициенты на 1win, советуем.
Играйте безопасно и выигрывайте большие деньги с 1win, рекомендуем.
1win беларусь 1win беларусь .
Приветствую. Подскажите, где почитать разные блоги о недвижимости? Сейчас читаю https://glwin.ru
Проекты домов Ижевск нк18.рф
Обращайтесь к нам за готовые дома под ключ ижевск на любом этапе застройки. У Вас уже имеется участок? Отлично, дом мы берем на себя. Определим все тонкости, дадим советы от специалистов по планировке. Участка пока нет? Мы предложим Вам несколько различных вариаций, которые подойдут определенно под Ваш спрос.
This article gives clear idea in support of the new viewers of blogging,
that truly how to do blogging and site-building.
Узаконивание самовольной перепланировки может показаться сложным процессом, но с нашей помощью это станет просто и быстро. Наша команда профессионалов знает все нюансы и готова помочь вам на каждом этапе.
Если вы не знаете, как узаконить самовольную перепланировку, обращайтесь к нам. Мы обеспечим полное сопровождение процесса, начиная с подготовки документов и заканчивая получением всех разрешений. С нами вы легко решите все вопросы и получите законное пространство для жизни или работы.
Приветствую. Может кто знает, где почитать разные блоги о недвижимости? Пока нашел https://gor-bur.ru
Всем привет! Может кто знает, где почитать полезные блоги о недвижимости? Пока нашел https://hameleon1.ru
Многие собственники сталкиваются с вопросом, как узаконить перепланировку. Наша компания предлагает профессиональную помощь в легализации перепланировок, обеспечивая полное сопровождение процесса от начала до конца.
Процесс как узаконить перепланировку включает в себя подготовку документации, взаимодействие с жилищными инспекциями и другими органами. Мы гарантируем соблюдение всех требований законодательства и быстрое получение необходимых разрешений.
Приветствую. Подскажите, где найти разные статьи о недвижимости? Пока нашел https://iskrb.ru
Всем привет! Подскажите, где найти разные блоги о недвижимости? Сейчас читаю https://juzhnybereg24.ru
Приветствую. Может кто знает, где найти разные статьи о недвижимости? Пока нашел https://klimat-hck.ru
order tamoxifen
Приветствую. Может кто знает, где найти полезные блоги о недвижимости? Сейчас читаю https://kolahouse.ru
Doing so helps every individual speak about the problems that actually matter
and reduces tangential (and emotion-fueled) conversational muddle that has little bearing
on the conflict. The setting wherein a young individual grows up can have
a profound impact on their mental health. The technological wizards of the twenty first century have developed programs to help detect vehicles hanging out
in your blind spot and warn you to their presence.
So how can you avoid scams whereas getting probably the most out of your vehicle?
Приветствую. Может кто знает, где найтиразные блоги о недвижимости? Сейчас читаю https://sm70.ru
Всем привет! Может кто знает, где найти разные блоги о недвижимости? Сейчас читаю https://komdizrem.ru
Программа Медиагет поддерживает работу на различных операционных системах, включая Windows. Узнайте о системных требованиях на https://skachat-mediaget-fast.ru.
You will bear in mind that you just messed up in the event
you get unfavorable comments from a clientele.
Admirable feedbacks are extremely gratifying nonetheless the paradox can be poor comments are virus-like and much of people are usually affected simply by a small
unfavorable evaluate. The recommendations are required to
produce a constructive feeling for the Web site browser.
Приветствую. Может кто знает, где найти полезные блоги о недвижимости? Пока нашел https://konditsioneri-shop.ru
Приветствую. Подскажите, где найти полезные статьи о недвижимости? Пока нашел https://glatt-nsk.ru
Thank you for great content. Hello Administ. Seo Paketi Skype: By_uMuT@KRaLBenim.Com -_- live:by_umut
Thank you great post. Hello Administ .Seo Paketi Skype: By_uMuT@KRaLBenim.Com -_- live:by_umut
After all, what a great site and informative posts, I will upload inbound link – bookmark this web site? Regards, Reader.Seo Paketi Skype: By_uMuT@KRaLBenim.Com -_- live:by_umut
Thank you for great article. Hello Administ .Seo Paketi Skype: By_uMuT@KRaLBenim.Com -_- live:by_umut
Hi, just required you to know I he added your site to my Google bookmarks due to your layout. But seriously, I believe your internet site has 1 in the freshest theme I??ve came across.Seo Paketi Skype: By_uMuT@KRaLBenim.Com -_- live:by_umut
Thank you for great article. Hello Administ .Seo Paketi Skype: By_uMuT@KRaLBenim.Com -_- live:by_umut
Everything is very open and very clear explanation of issues. was truly information.Seo Paketi Skype: By_uMuT@KRaLBenim.Com -_- live:by_umut
Good info. Lucky me I reach on your website by accident, I bookmarked it. Seo Paketi Skype: By_uMuT@KRaLBenim.Com -_- live:by_umut
Thank you for content. Area rugs and online home decor store. Hello Administ . Seo Paketi Skype: By_uMuT@KRaLBenim.Com -_- live:by_umut
Thank you for great content. Hello Administ. Seo Paketi Skype: By_uMuT@KRaLBenim.Com -_- live:by_umut
Hi, just required you to know I he added your site to my Google bookmarks due to your layout. But seriously, I believe your internet site has 1 in the freshest theme I??ve came across.Seo Paketi Skype: By_uMuT@KRaLBenim.Com -_- live:by_umut
Great post thank you. Hello Administ . Seo Paketi Skype: By_uMuT@KRaLBenim.Com -_- live:by_umut
Everything is very open and very clear explanation of issues. was truly information.Seo Paketi Skype: By_uMuT@KRaLBenim.Com -_- live:by_umut
Everything is very open and very clear explanation of issues. was truly information.Seo Paketi Skype: By_uMuT@KRaLBenim.Com -_- live:by_umut
Мультимедийный интегратор Мультимедийный интегратор .
Имея в виду еда на заказ с доставкой заходите на указанный веб ресурс. На сайте можно увидеть наше меню, сделать заказ, заказать столик или позвонить нам. Контактный телефон +7(3412)223-225 или делайте заказ сразу на сайте. В тематике «доставка готовых блюд» откроется наше полное меню. Обратите своё внимание на оформление блюда при заказе, это настоящее искусство. Приготовление также у нас нестандартное, следовательно можете не переживать перед заказом на особенный вечер.
Самая лучшая еда тут – доставка еды приходите прямо сейчас. Мы находимся по адресу: г. Ижевск, ул. Максима Горького, д. 163. Режим работы с 12:00 до 00:00, а в пятницу и субботу до 2-х ночи. Приглашаем Вас и Вашу половинку великолепно провести время или оформить заказ на restoyar.ru на дом и насладиться вкусной кухней в своей знакомой атмосфере.
prednisone 20 mg over the counter
Всем привет! Может кто знает, где найти полезные блоги о недвижимости? Пока нашел вот
buy azithromycin uk
видеостена купить москва видеостена купить москва .
Spot on with this write-up, I seriously believe that this
amazing site needs a great deal more attention. I’ll probably be returning to see more, thanks for the advice!
where can i buy albuterol over the counter
СОУТ заказать москва
Обеспечение надежных условий работы — это не только выполнение нормативов, но также забота о здоровье и благополучии работников. Специальная оценка условий труда способствует выявлению и устранению опасностей, что ведет к снижению уровня травматизма и повышению эффективности работы. Обращайтесь в Safety Systems Group, чтобы создать безопасные условия для своих сотрудников и улучшить атмосферу в коллективе.
Thanks for sharing. I read many of your blog posts, cool, your blog is very good.
озвучивание https://ozvuchivanie-pomeshhenij.ru/ .
магазин аккаунтов инстаграм https://magazin-akkauntov.ru/ .
Нужен переводчик, который работает везде? Загляните на https://teletype.in/@golosai/kakoi-perevodchik-rabotaet-bez-interneta и узнайте о приложениях, не требующих подключения к интернету. Общайтесь свободно, где бы вы ни были!
Думаете, что знаете все о том, как ответить на “Купи слона”? Проверьте свои знания на https://teletype.in/@golosai/kupi-slona-kak-otvetit. Возможно, вы откроете для себя новые, неожиданные способы ответа, которые удивят даже самых опытных “слоновых” игроков.
Специальная оценка условий труда
Создание безопасных условий труда — это не только соблюдение нормативных требований, но также забота о здоровье и благополучии работников. Специальная оценка безопасных условий труда способствует выявлению и устранению опасностей, что уменьшает травматизм и повышает рабочую эффективность. Обращайтесь в Safety Systems Group, чтобы создать безопасные условия для своих сотрудников и улучшить атмосферу в коллективе.
synthroid 100 mg coupon
hello!,I like your writing very much! share we communicate more about your article on AOL? I require an expert on this area to solve my problem. Maybe that’s you! Looking forward to see you.
Всем привет! Подскажите, где найтиразные блоги о недвижимости? Пока нашел https://krovli-12.ru
amoxicillin 500 mg tablets cost
modafinil price australia
What’s Happening i’m new to this, I stumbled upon this I have found It absolutely helpful and it has aided me out loads. I hope to contribute & help other users like its helped me. Great job.
I am very happy to read this. This is the kind of manual that needs to be given and not the accidental misinformation that is at the other blogs. Appreciate your sharing this greatest doc.
Всем привет! Подскажите, где почитатьразные статьи о недвижимости? Сейчас читаю https://varmex-spb.ru
It’s actually a cool and useful piece of information. I’m glad that you shared this helpful info with us. Please keep us up to date like this. Thanks for sharing.
It is truly a nice and useful piece of info. I’m glad that you simply shared this useful info with us. Please keep us informed like this. Thanks for sharing.
It is also frequent for American coins to be discovered among circulation as a result of shut proximity to the United States and the fact that
the sizes and colours of the coins are related. The Home
of Wettin dominated Poland-Lithuania and Saxony simultaneously, dividing power between the 2 states.
Two such rugs have been ordered for the foyer entrance, each
measuring 27 by 48 ft (8.2 by 14.6 m).
Contortion actually emerged as a performance act with
the institution of the Mongolian State Circus in 1941, which introduced its first official contortionist, Tsend-ayush.
It was commissioned by Eaux Claires Festival and made its
world premiere in 2015 where it served as the official place to begin of
the festival on each Friday and Saturday.
dexamethasone tablet price
Если вы не нашли нужное приложение в каталоге Яндекс ТВ, попробуйте использовать функцию поиска. Введите название приложения в строку поиска и нажмите “Найти”. Если приложение доступно, оно появится в результатах поиска. Выберите его и следуйте инструкциям по установке. Больше информации о поиске и установке приложений: https://teletype.in/@golosai/kak-ustanovit-prilozhenie-na-iandeks-tv
Thank you for your sharing. I am worried that I lack creative ideas. It is your article that makes me full of hope. Thank you. But, I have a question, can you help me?
I loved as much as you will receive carried out right here.
The sketch is tasteful, your authored subject matter stylish.
nonetheless, you command get got an edginess over that you
wish be delivering the following. unwell unquestionably come further formerly again since
exactly the same nearly very often inside case you shield this increase.
0.8%. Different important Asian American teams include Cambodian, Laotian, Hmong, Taiwanese, Pakistani,
and Thai People. Asians of non-Hispanic origin make up
13.8% of the population, about 1.4% South Asian (Indian Subcontinent), and about 12.4% have been East or Southeast Asian.
I like this post, enjoyed this one thankyou for putting up.
I’ll right away grasp your rss as I can not find your e-mail subscription hyperlink or newsletter service. Do you have any? Please let me recognize so that I may subscribe. Thanks.
Всем привет! Может кто знает, где почитать полезные блоги о недвижимости? Сейчас читаю https://konditsioneri-shop.ru
Лучшие автомобили из Кореи | Секреты выбора авто из Кореи | Свежие поступления авто из Кореи | Самые популярные авто Кореи | Почему стоит выбрать корейский автомобиль? | Топ-3 востребованных автомобиля из Кореи | Корейские автомобили с выгодным расходом топлива | Лучшие по соотношению цена-качество корейские авто | Выбор лучшего корейского автомобиля | Корейские SUV: особенности моделей | Как правильно страховать авто из Кореи? | Корейские авто для долгих поездок: комфорт и безопасность | Как выбрать городской автомобиль из Кореи? | Как оценить состояние авто из Кореи перед покупкой? | Как сделать уникальным свой корейский автомобиль
автомобили из кореи https://avtodom63.ru/ .
Услуги невролога Москва cecilplus.ru
Если Вы искали врач акушер гинеколог москва в интернете, то вы на нужном пути. Наши врачи на cecilplus.ru обязательно Вам окажут помощь, ведь у них огромный опыт и постоянные повышения в своей сфере. Будем рады Вам помочь обрести здоровое тело, побороть болезнь и жить счастливой жизнью!
Стоимость ээг в Москве ребенку cecilplus.ru
Если Вы хотели найти медицинский центр гинекология в сети интернет, то вы на нужном пути. Наши врачи на cecilplus.ru непременно Вам окажут помощь, ведь у них большой опыт и постоянные повышения квалификации. Будем счастливы Вам оказать помощь обрести здоровье, побороть недуг и жить счастливой жизнью!
Если в вашем доме есть совет жильцов или старший по подъезду, обратитесь к ним. Они обычно владеют информацией о коде домофона и могут вам помочь. О роли жильцов в обеспечении безопасности дома рассказывается в статье https://teletype.in/@golosai/kak-uznat-kod-domofona-v-svoem-podieezde.
baclofen 25 mg tablet
современный конференц зал http://www.oborudovanie-dlja-konferenc-zalov.ru/ .
트레져스 오브 아즈텍
“무슨 말이야?” Yang Biao는 잘 이해하지 못한 채 주위를 둘러 보았습니다.
рейтинг прогнозистов http://www.rejting-kapperov12.ru/ .
price of generic provigil
I love your blog.. very nice colors & theme.
Did you make this website yourself or did you hire someone to do it for you?
Plz reply as I’m looking to construct my own blog and would like to
find out where u got this from. cheers
I’ll right away seize your rss feed as I can not find your e-mail subscription hyperlink
or e-newsletter service. Do you have any? Kindly allow me know in order that I may
just subscribe. Thanks.
Havemann. L. (2020). Open within the evening: Openings and closures in an ecology of practices.
Nusbaum, Amy T. (2020). “Who Will get to Wield Educational Mjolnir?: On Worthiness, Knowledge Curation, and Utilizing the ability of the Individuals to Diversify OER”.
Sanchez, Claudia. “The usage of technological sources for education: a new professional competency for teachers”.
Over 90% of the world’s mining workforce are engaged in ASM, with an estimated 40.5 million individuals immediately
engaged in ASM, from over eighty international locations in the
global south. More than 150 million people indirectly depend on ASM for their livelihood.
Записать на прием к гинекологу Москва cecilplus.ru
По поводу урология цены мы Вам с удовольствием окажем помощь. Предлагаем консультации, лечение и диагностику по различным направлениям. В их числе: геронтология, терапия, невролгия-алгология, ревматология, педиатрия и многие другие. По возникшим вопросам звоните по номеру телефона +7(499)705-04-19 или оформите обратный звонок на веб портале cecilplus.ru уже сейчас. Ещё есть интернет запись и оплата приема для Вашего удобства.
buy baclofen 50mg
помещение для переговоров http://oborudovanie-dlja-peregovornoj-komnaty.ru/ .
оборудование конференц залов оборудование конференц залов .
помещение для переговоров oborudovanie-peregovornyh-komnat.ru .
Your point of view caught my eye and was very interesting. Thanks. I have a question for you.
lcd видеостена москва https://videosteny-dlja-sozdanija-jekranov.ru/ .
оборудование актового зала оборудование актового зала .
amoxicillin 8500 mg
оборудование для актового зала оборудование для актового зала .
cheap accutane online
advair 500 coupon
generic vermox cheap